Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
6 Skeletal System
6.1 Introduction
In this chapter, you will learn about the structure, functions, growth, repair, and disorders of the skeletal system. Specifically you will learn about:
The components of the skeletal system, which includes bones, ligaments, and cartilage.
The functions of the skeletal system, including supporting and giving shape to the body; protecting internal organs; facilitating movement; producing blood cells; helping maintain homeostasis; and producing endocrine hormones.
The organization and functions of the two main divisions of the skeletal system: the axial skeletal system (which includes the skull, spine, and rib cage), and the appendicular skeletal system (which includes the limbs and girdles that attach the limbs to the axial skeleton).
The tissues and cells that make up bones, along with their specific functions, which include making new bone, breaking down bone, producing blood cells, and regulating mineral homeostasis.
The different types of bones in the skeletal system, based on shape and location.
How bones grow, remodel, and repair themselves.
The different types of joints between bones, where they are located, and the ways in which they allow different types of movement, depending on their structure.
The causes, risk factors, and treatments for the two most common disorders of the skeletal system — osteoporosis and osteoarthritis.
6.2 THE SKELETAL SYSTEM
Figure 6.1 Bones can be quite jolly.
SKULL AND CROSS-BONES
The skull and crossbones symbol has been used for a very long time to represent death, perhaps because after death and decomposition, bones are all that remain. Many people think of bones as dead, dry, and brittle. These adjectives may correctly describe the bones of a preserved skeleton, but the bones of a living human being are very much alive. Living bones are also strong and flexible. Bones are the major organs of the skeletal system.
OVERVIEW OF THE SKELETON SYSTEM
The skeletal system is the organ system that provides an internal framework for the human body. Why do you need a skeletal system? Try to imagine what you would look like without it. You would be a soft, wobbly pile of skin containing muscles and internal organs, but no bones. You might look something like a very large slug. Not that you would be able to see yourself — folds of skin would droop down over your eyes and block your vision, because of your lack of skull bones. You could push the skin out of the way, if you could only move your arms, but you need bones for that, as well!
COMPONENTS OF THE SKELETAL SYSTEM
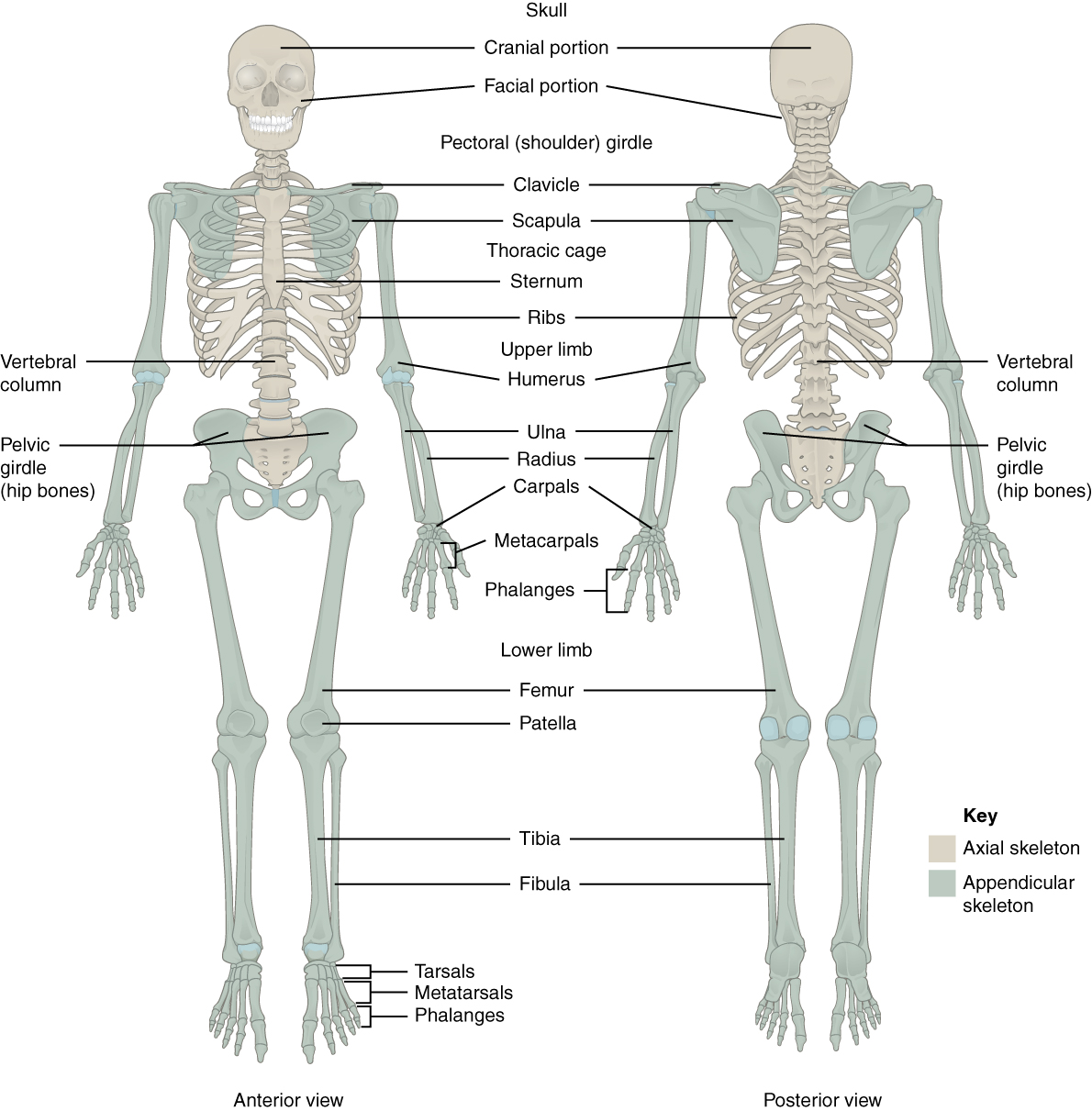
In adults, the skeletal system includes 206 bones, many of which are shown in Figure 6.2 below. Bones are organs made of supportive connective tissues, mainly the tough protein collagen. Bones contain blood vessels, nerves, and other tissues, and they are hard and rigid, due to deposits of calcium and other mineral salts within their living tissues. Spots where two or more bones meet are called joints. Many joints allow bones to move like levers. Your elbow, for example, is a joint that allows you to bend and straighten your arm.
Figure 6.2 The adult skeleton contains 206 bones. A newborn infant has 270 bones, but many of them fuse together by adulthood.
Besides bones, the skeletal system includes cartilage and ligaments.
Cartilage is a type of dense connective tissue, made of tough protein fibers. It is strong, but flexible and very smooth. It covers the ends of bones at joints, providing a smooth surface for bones to move over.
Ligaments are bands of dense fibrous connective tissue that hold bones together. They keep the bones of the skeleton in place.
AXIAL AND APPENDICULAR SKELETONS
The skeleton is traditionally divided into two major parts: the axial skeleton and the appendicular skeleton, both of which are pictured below (Figure 6.3 and Figure 6.4 respectively).
The axial skeleton forms the axis of the body. It includes the skull, vertebral column (spine), and rib cage. The bones of the axial skeleton — along with ligaments and muscles — allow the human body to maintain its upright posture. The axial skeleton also transmits weight from the head, trunk, and upper extremities down the back to the lower extremities. In addition, the bones protect the brain and organs in the chest.
Figure 6.3 The axial skeleton.
The appendicular skeleton forms the appendages and their attachments to the axial skeleton. It includes the bones of the arms and legs, hands and feet, and shoulder and pelvic girdles. The bones of the appendicular skeleton make possible locomotion and other movements of the appendages. They also protect the major organs of digestion, excretion, and reproduction.
Figure 6.4 The appendicular skeleton.
FUNCTIONS OF THE SKELETAL SYSTEM
The skeletal system has many different functions that are necessary for human survival. Some of the functions, such as supporting the body, are relatively obvious. Other functions are less obvious but no less important. Three tiny bones (hammer, anvil, and stirrup) inside the middle ear, for example, transfer sound waves into the inner ear.
SUPPORT, SHAPE, AND PROTECTION
The skeleton supports the body and gives it shape. Without the rigid bones of the skeletal system, the human body would be just a bag of soft tissues, as described above. The bones of the skeleton are very hard and provide protection to the delicate tissues of internal organs. For example, the skull encloses and protects the soft tissues of the brain, and the vertebral column protects the nervous tissues of the spinal cord. The vertebral column, ribcage, and sternum (breastbone) protect the heart, lungs, and major blood vessels. Providing protection to these latter internal organs requires the bones to be able to expand and contract. The ribs and the cartilage that connects them to the sternum and vertebrae are capable of small shifts that allow breathing and other internal organ movements.
MOVEMENT
Figure 6.5 Bones that meet at the elbow and shoulder joint include the scapula, humerus, radius and ulna. These bones provide attachment surfaces for muscles that move the bones at the joint.
The bones of the skeleton provide attachment surfaces for skeletal muscles. When the muscles contract, they pull on and move the bones. Figure 6.5, for example, shows the muscles attached to the bones at the elbow and shoulder. They help stabilize the joint and allow the arm to bend at these two joints. The bones at joints act like levers moving at a fulcrum point, and the muscles attached to the bones apply the force needed for movement.
HEMATOPOIESIS
Hematopoiesis is the process by which blood cells are produced. This process occurs in a tissue called red marrow, which is found inside some bones. Red marrow synthesizes red blood cells, white blood cells, and platelets. Billions of these blood cells are produced inside the bones every day.
MINERAL STORAGE AND HOMEOSTASIS
Another function of the skeletal system is storing minerals, especially calcium and phosphate. This storage function is related to the role of bones in maintaining mineral homeostasis. Just the right levels of calcium and other minerals are needed in the blood for normal functioning of the body. When mineral levels in the blood are too high, bones absorb some of the minerals and store them as mineral salts, which is why bones are so hard. When blood levels of minerals are too low, bones release some of the minerals back into the blood. Bone minerals are alkaline (basic), so their release into the blood buffers the blood against excessive acidity (low pH), whereas their absorption back into bones buffers the blood against excessive alkalinity (high pH). In this way, bones help maintain acid-base homeostasis in the blood.
Another way that bones help maintain homeostasis is by acting as an endocrine organ. One endocrine hormone secreted by bone cells is osteocalcin, which helps regulate blood glucose and fat deposition. It increases insulin secretion, as well as cell’s sensitivity to insulin. In addition, it boosts the number of insulin-producing cells and reduces fat stores.
SEXUAL DIMORPHISM OF THE HUMAN SKELETON
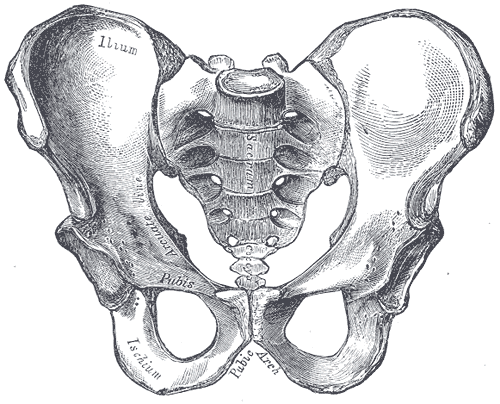
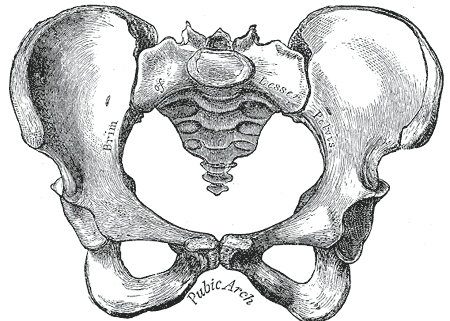
The human skeleton is not as sexually dimorphic as that of many other primate species, although human female skeletons tend to be smaller and less robust than human male skeletons within a given population. There are also subtle differences between males and females in the morphology of the skull, teeth, longs bones, and pelvis. The greatest difference is in the pelvis, because the female pelvis is adapted for childbirth. Take a look at the pelvises in Figure 6.6 and 6.7. How are they different?
Figure 6.6 The male pelvis.
Figure 6.7 The female pelvis
Review
What is the skeletal system? How many bones are there in the adult skeleton?
Describe the composition of bones.
Besides bones, what other organs are included in the skeletal system?
Identify the two major divisions of the skeleton.
List several functions of the skeletal system.
The female and male skeleton are identical. True or False.
What is a joint? How is cartilage related to joints? Identify one joint in the human body and describe its function.
6.3 DIVISIONS OF THE SKELETAL SYSTEM
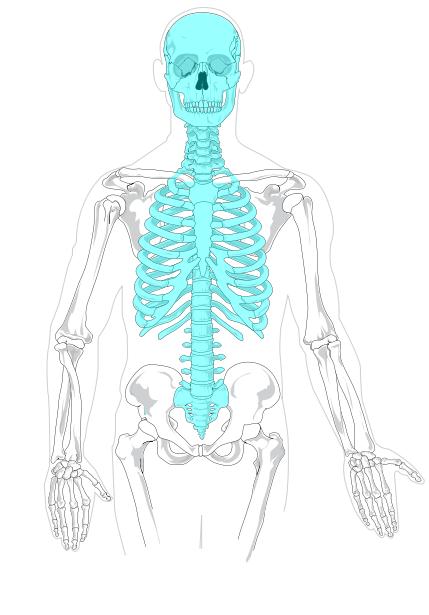
AXIAL SKELETON
Figure 6.8 The axial skeleton.
The axial skeleton, shown in blue in Figure 6.8, consists of a total of 80 bones. Besides the skull, it includes the rib cage and vertebral column. It also includes the three tiny ossicles (hammer, anvil, and stirrup) in the middle ear and the hyoid bone in the throat, to which the tongue and some other soft tissues are attached.
SKULL
The skull is the part of the human skeleton that provides a bony framework for the head. It consists of 22 different bones. There are eight bones in the cranium, which encloses the brain, and 14 bones in the face.
Cranium
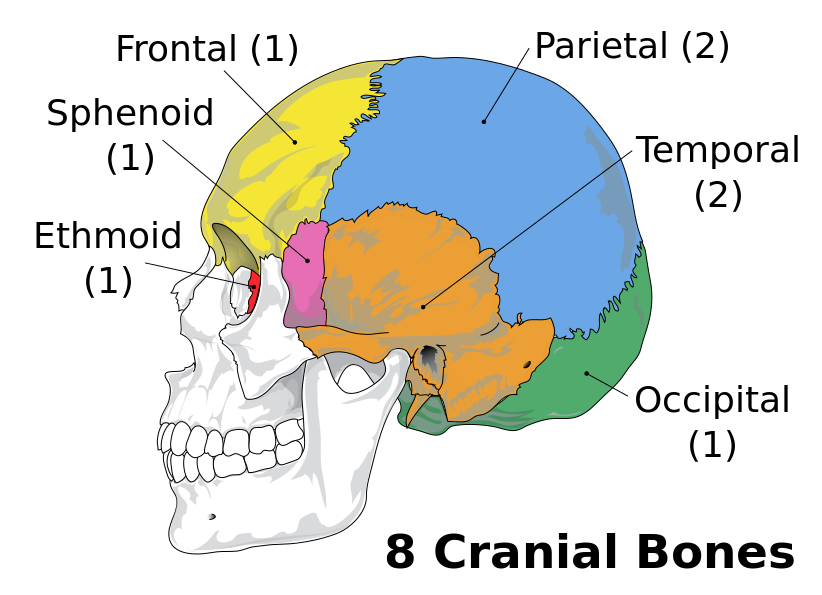
The cranium forms the entire upper portion of the skull. As shown in Figure 6.8, it consists of eight bones: one frontal bone, two parietal bones, two temporal bones, one occipital bone, one sphenoid bone, and one ethmoid bone. The ethmoid bone separates the nasal cavity from the brain. The sphenoid bone is one of several bones, including the frontal bone, that help form the eye sockets. The other bones of the cranium are large and plate-like. They cover and protect the brain. The bottom of the skull has openings for major blood vessels and nerves. A large opening, called the foramen, connects the spinal cord and brain.
Figure 6.9 The cranium consists of eight bones that are fused together at their joints.
Facial Bones
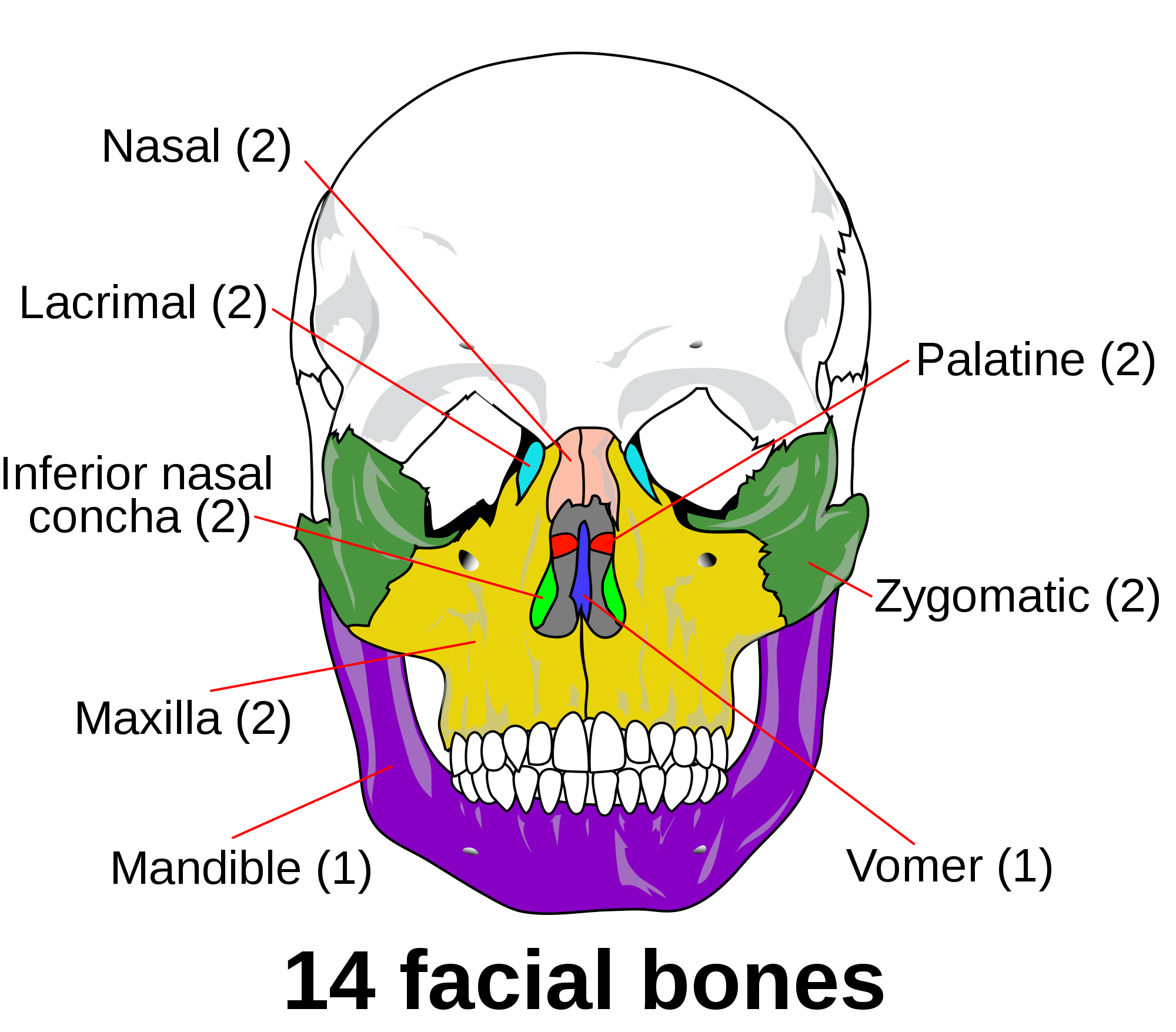
The 14 facial bones of the skull are located below the frontal bone of the cranium, and they are depicted in Figure 6.10. Large bones in the face include the upper jaw bones, or maxillae(singular, maxilla), which form the middle part of the face and the bottom of the two eye sockets. The maxillae are fused together, except for an opening between them for the nose. The lower edge of the maxillae contains sockets for the upper teeth. The lower jawbone, or mandible, is also large. The top edge of the mandible contains sockets for the lower teeth. The mandible opens and closes to chew food and is controlled by strong muscles. There are two zygomatic (or cheek) bones and two nasal bones. The nasal region also contains seven smaller bones, as indicated in Figure 6.9.
Figure 6.10 The 14 bones that make up the face are labeled in this drawing of the skull.
VERTEBRAL COLUMN
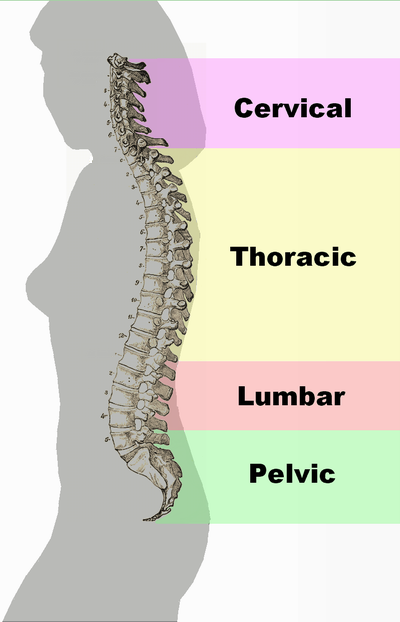
Figure 6.11 The vertebral column consists of 24 individual vertebrae that are separated by intervertebral discs of cartilage. An additional nine vertebrae are fused together at the base of the spine. Note the S-shaped curve of the vertebral column in the profile view on the right.
The vertebral column — also called the spine or backbone — is the flexible column of vertebrae (singular, vertebra) that connects the trunk with the skull and encloses the spinal cord. It consists of 33 vertebrae that are divided into five regions, as shown in Figure 6.11: the cervical, thoracic, lumbar, sacral and coccygeal regions. From the neck down, the first 24 vertebrae (cervical, thoracic, and lumbar) are individual bones. The five sacral vertebrae are fused together, as are the four coccygeal vertebrae.
The vertebral column consists of 24 individual vertebrae that are separated by intervertebral discs of cartilage. An additional nine vertebrae are fused together at the base of the spine. Note the S-shaped curve of the vertebral column in the profile view in Figure 6.10 on the left.
The human vertebral column reflects adaptations for upright bipedal locomotion (walking upright on two legs). For example, the vertebral column is less like a rigid column than an S-shaped spring. Although newborn infants have a relatively straight spine, the curves develop as the backbone starts taking on its support functions, such as keeping the trunk erect, holding up the head, and helping to anchor the limbs. The S shape of the vertebral column allows it to act like a shock absorber, absorbing much of the jarring of walking and running so the forces are not transmitted directly from the pelvis to the skull. The S shape also helps protect the spine from breaking, which would be more likely with a straight, more rigid vertebral column. In addition, the S shape helps to distribute the weight of the body — particularly of the internal organs, so the weight load is not all at the bottom, as would occur with a straight spine.
RIB CAGE
The rib cage (also called thoracic cage) is aptly named, because it forms a sort of cage that holds within it the organs of the upper part of the trunk, including the heart and lungs. It is shown in Figures 6.12-6.14. The rib cage includes the 12 thoracic vertebrae and the sternum, as well as 12 pairs of ribs, which are attached at joints to the vertebrae. The ribs are divided into three groups, called true ribs, false ribs, and floating ribs. The top seven pairs of ribs are true ribs. They are attached by cartilage directly to the sternum. The next three pairs of ribs are false ribs. They are attached by cartilage to the ribs above them, rather than directly to the sternum. The lowest two pairs of ribs are floating ribs. They are attached by cartilage to muscles in the abdominal wall. The attachments of false and floating ribs let the lower part of the rib cage expand to accommodate the internal movements of breathing.
Figure 6.12 True ribs are attached to both the vertebrae and the sternum. In this image, true ribs are highlighted in red.
Figure 6.13 False ribs are attached to the vertebrae and to the ribs above them by cartilage. In this image, false ribs and floating ribs are highlighted in red.
Figure 16.14 Floating ribs are attached to vertebrae and the muscles in the abdominal wall. In this image floating ribs are highlighted in red.
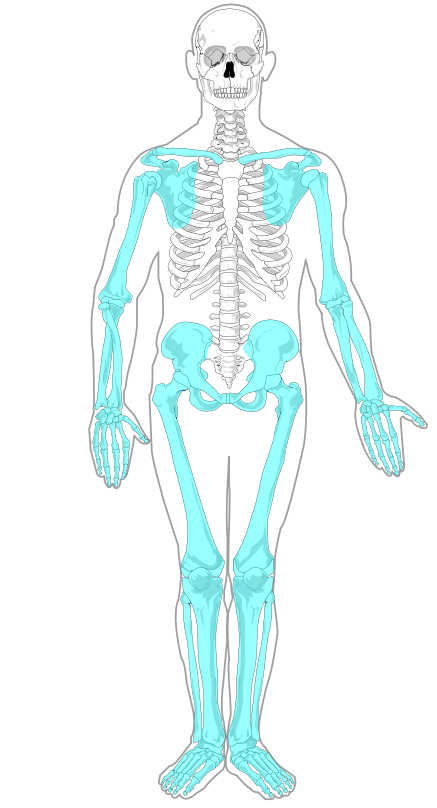
Appendicular Skeleton
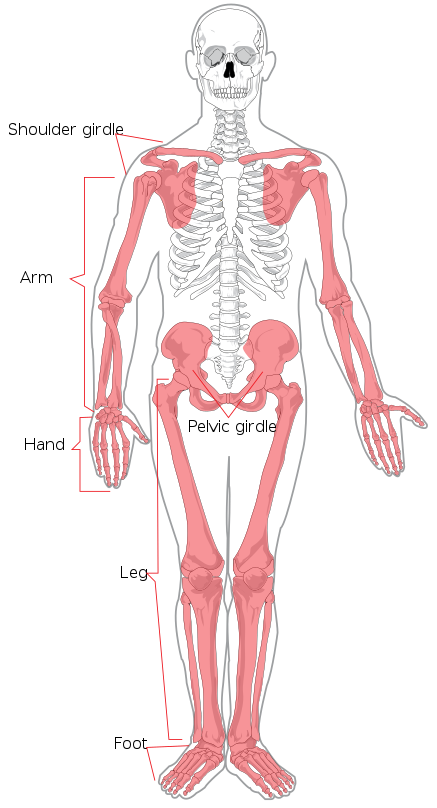
The appendicular skeleton, shown in red (Figure 6.15), consists of a total of 126 bones. It includes all the bones of the limbs (arms, legs, hands, and feet,) as well as the bones of the shoulder (shoulder girdle) and pelvis (pelvic girdle).
Figure 6.15 The appendicular skeleton includes the upper and lower appendages and girdles.
UPPER LIMBS
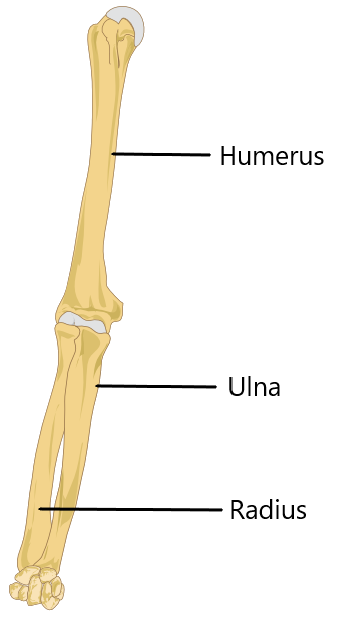
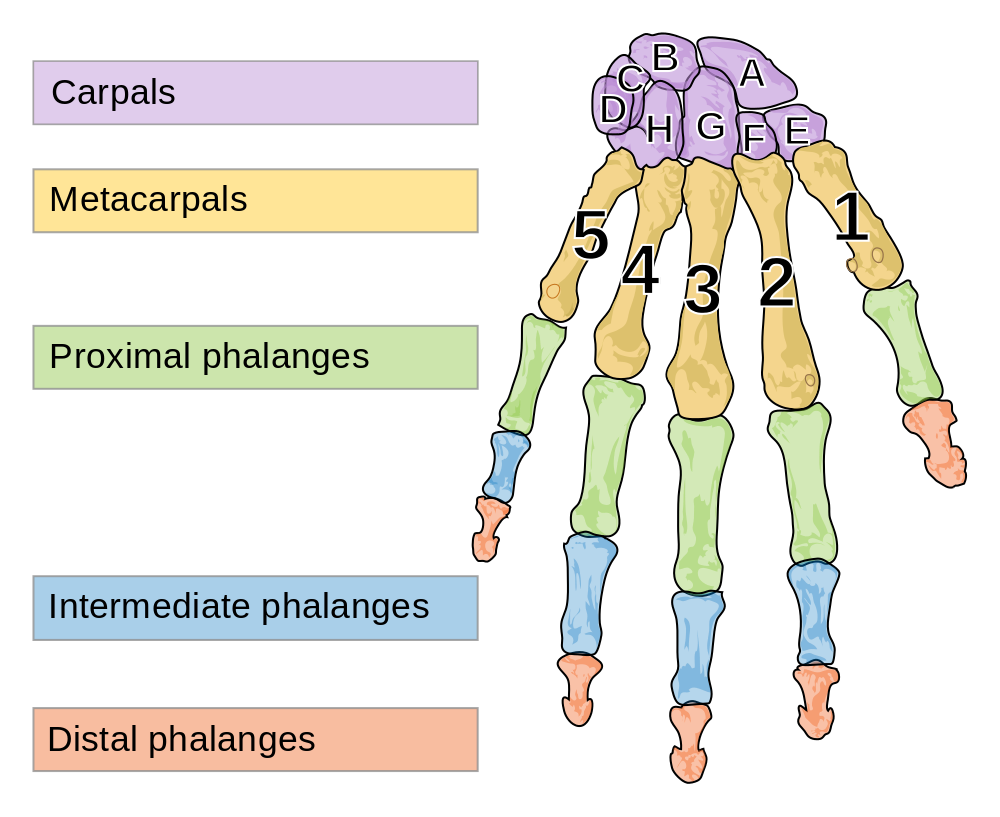
Each upper limb consists of 30 bones. As shown in Figure 6.16, there is one bone (called the humerus) in each of the upper arms, and there are two bones (called the ulna and radius) in each of the lower arms. The remaining bones of the upper limb are shown in Figure 6.16. Each wrist contains eight carpal bones — which are arranged in two rows of four bones each — and each hand contains five metacarpal bones. The bones in the fingers of each hand include 14 phalanges (three in each finger except the thumb, which has two phalanges). The thumb has the unique ability to move into opposition with the palm of the hand, and with each of the fingers when they are slightly bent. This allows the hand to handle and manipulate objects such as tools.
Figure 6.17The arm consists of three bones: the humerus, radius and ulna.Figure 6.16 Bones of the wrist (carpals A-E) and hand (metacarpals 1-5 and phalanges).
LOWER LIMBS
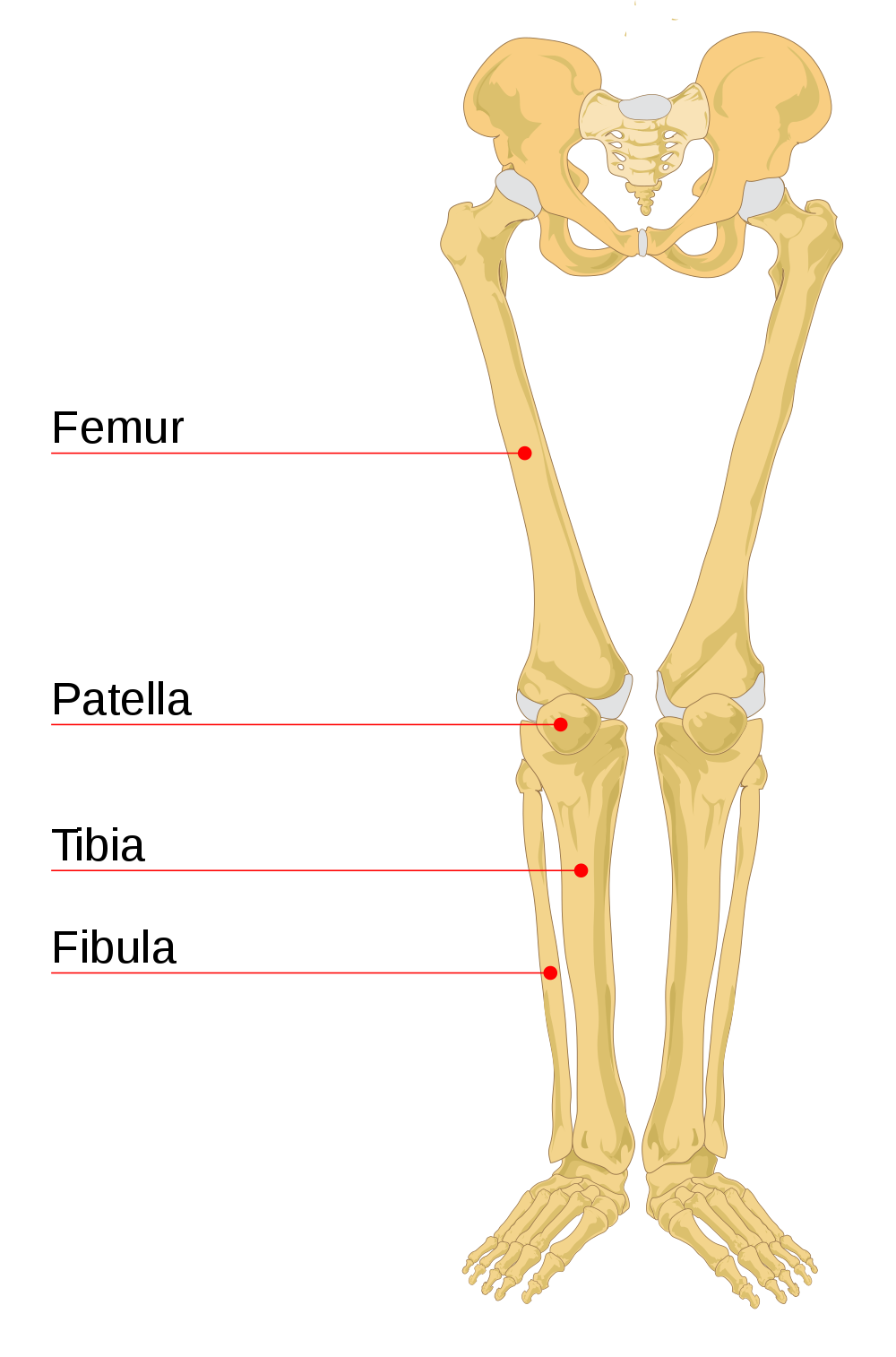
Figure 6.18 Bones of the legs.
Each lower limb consists of 30 bones. As shown in Figure 6.18 to the left, there is one bone (called the femur) in each of the upper legs, and there are two bones (called the tibia and fibula) in each of the lower legs. The kneecap (or patella) is an additional leg bone at the front of each knee, which is the largest joint in the human body.
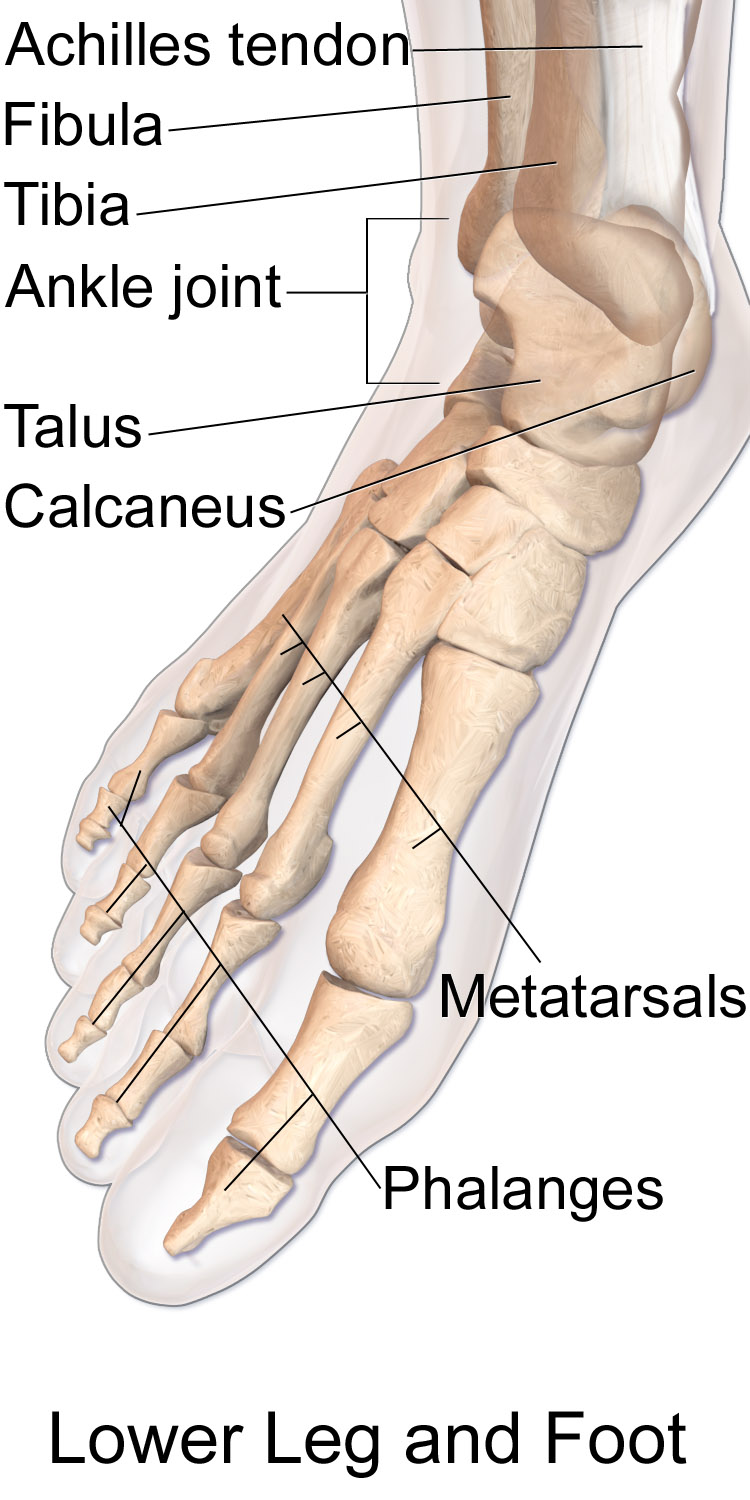
Figure 6.19 Bones of the lower leg (fibula and tibia), ankle (talus), heel (calcaneus), foot (metatarsals), and toes (phalanges).
The remaining bones of the lower limbs are in Figure 6.19 to the right. Each ankle contains seven tarsal bones (including the talus and calcaneus), and each foot contains five metatarsal bones. The tarsals and metatarsals form the ankle, heel, and arch of the foot. They give the foot strength while allowing flexibility. The bones in the toes of each foot consist of 14 phalanges (three in each toe except the big toe, which has two phalanges)
Bones of the lower leg (fibula and tibia), ankle (talus), heel (calcaneus), foot (metatarsals), and toes (phalanges)
SHOULDER GIRDLE
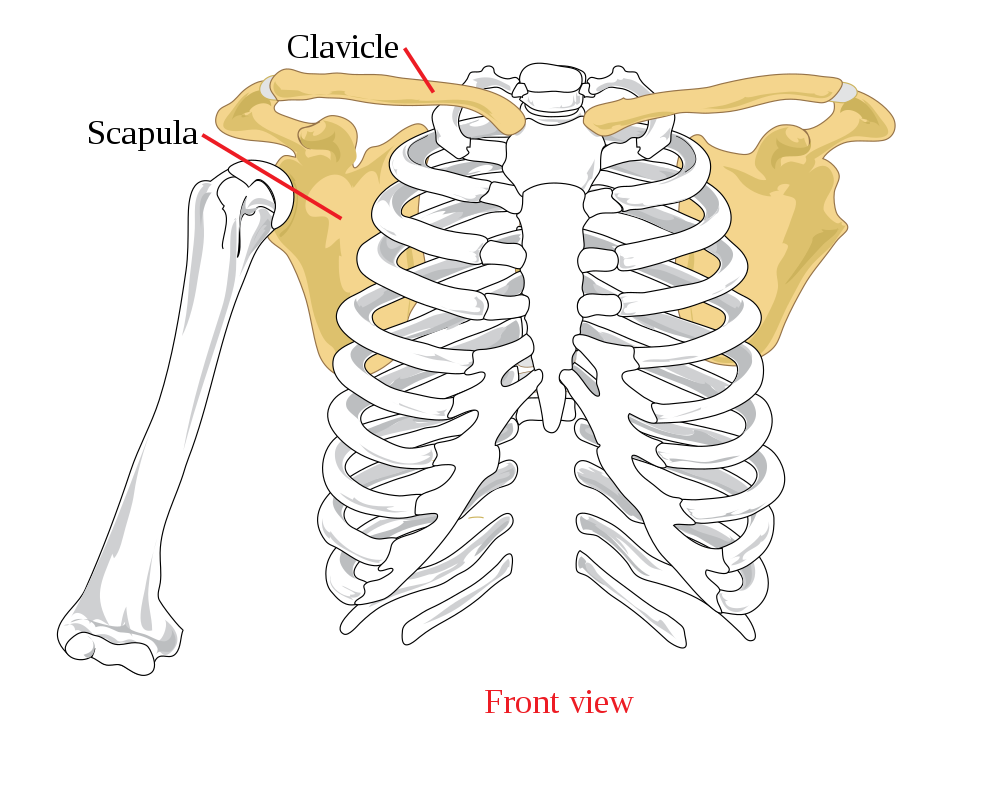
The pectoral girdle (also called shoulder girdle) attaches the upper limbs to the trunk of the body. It is connected to the axial skeleton by muscles alone. This allows a considerable range of motion in the upper limbs. The shoulder girdle consists of just two pairs of bones, with one of each pair on opposite sides of the body (see Figure 6.20). There are a right and left clavicle (collarbone), and a right and left scapula (shoulder blade). The scapula is a pear-shaped flat bone that helps form the shoulder joint. The clavicle is a long bone that serves as a strut between the shoulder blade and the sternum.
Figure 6.20 Bones of the shoulder girdle.
Pelvic Girdle
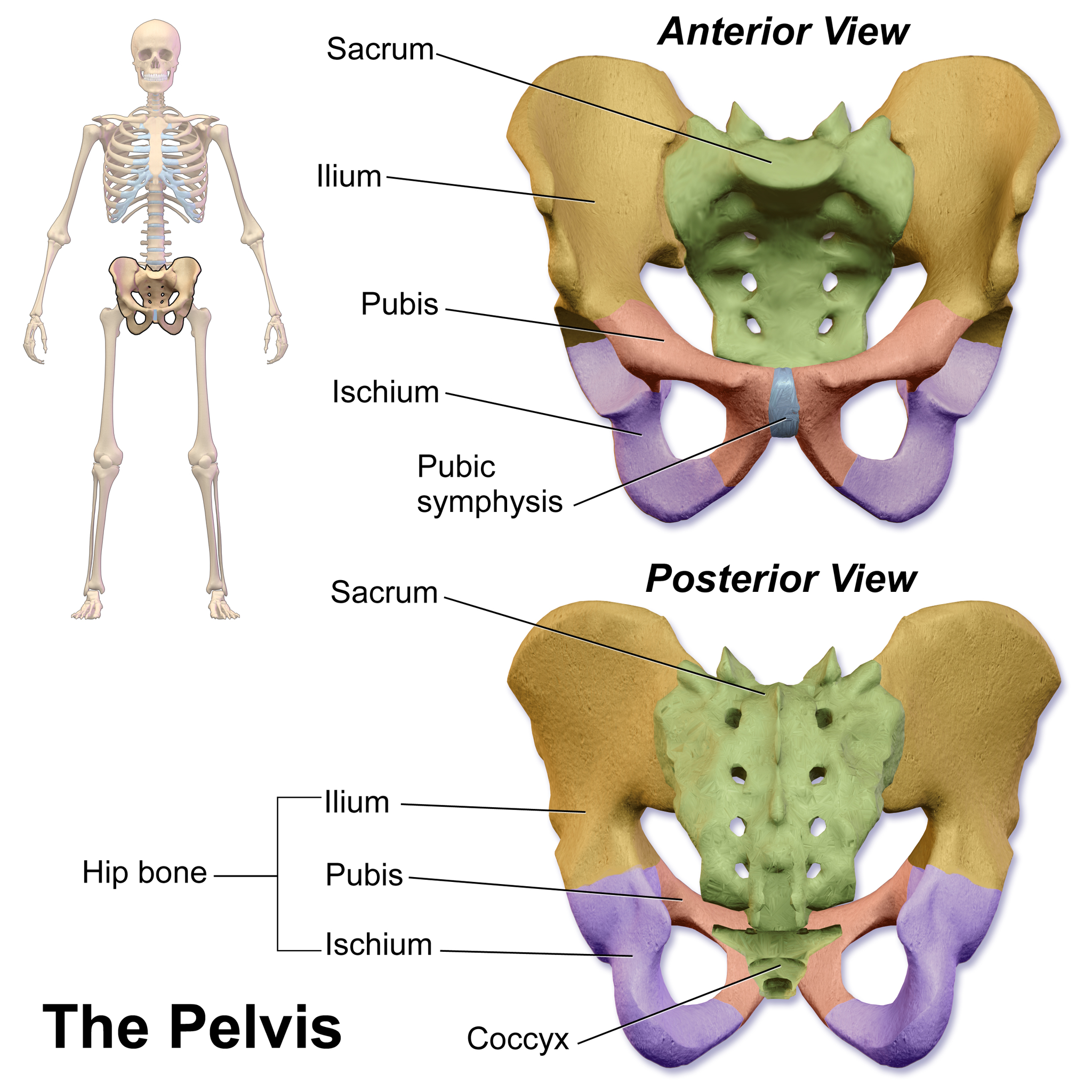
Figure 6.21 Bones of the pelvic girdle.
The pelvic girdle attaches the legs to the trunk of the body, and also provides a basin to contain and support the organs of the abdomen. It is connected to the vertebral column of the axial skeleton by ligaments. The pelvic girdle consists of two halves — one half for each leg — but the halves are fused with each other in adults at a joint called the pubic symphysis. Each half of the pelvic girdle is made up of two coxal bones. Each includes three bones, as shown in Figure 6.21 to the right: the ilium (flaring upper part of the pelvic girdle), pubis (lower front), and ischium (lower back). Each of these bones helps form the acetabulum, which is a depression into which the top of the femur (thighbone) fits. When the body is in a seated position, it rests on protrusions (called tuberosities) of the two ischial bones.
Review
Which bones are part of the axial skeleton? Which bones are part of the appendicular skeleton?
Fill in the blanks. The upper portion of the skull, called the consists of 8 bones. The bone that makes up your forehead is calls the bone. The bone at the very base of your skull is called your bone. The bones below the frontal bone are called the bones of which there are 14 bones. The two largest of these are the which is where you might grow a mustache, and the, more commonly called the jawbone.
What are the advantages of an S-shaped vertebral column?
What is the rib cage? What is its function? What types of ribs are there?
Explain the advantage of having some ribs that are not attached directly to the sternum.
What is the shoulder girdle? Why does it allow considerable upper limb mobility?
Describe some of the similarities between the upper limbs and the lower limbs.
Describe the pelvic girdle and the bones it contains.
Bones of the skull – Learn in 4 minutes! Neural Academy, 2018.
6.4 STRUCTURE OF BONE
WHAT ARE BONES?
Bones are organs that consist primarily of bone tissue, also called osseous tissue. Bone tissue is a type of connective tissue consisting mainly of a collagen matrix that is mineralized with calcium and phosphorus crystals. The combination of flexible collagen and hard mineral crystals makes bone tissue hard, without making it brittle.
BONE ANATOMY
There are several different types of tissues in bones, including two types of osseous tissues. Osseous tissues, in turn, consist of several different types of bone cells.
TYPES OF OSSEOUS TISSUE
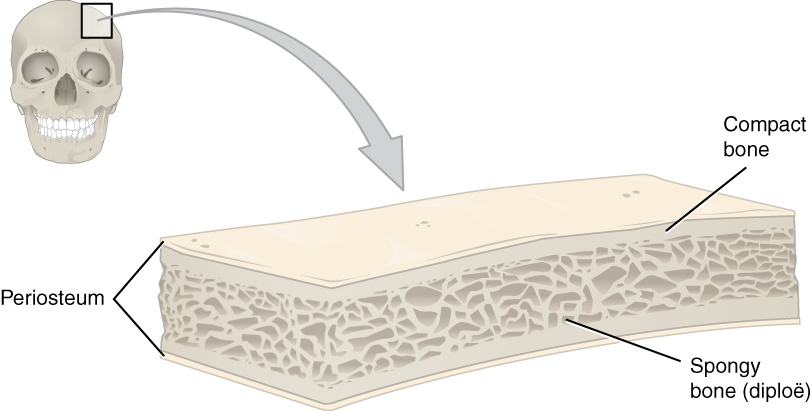
The two different types of osseous tissue are compact bone tissue (also called hard or cortical bone) and spongy bone tissue (also called cancellous or trabecular bone). Both are shown in the diagrams of a typical bone in Figures 6.22 and 6.23.
Flat bones are typically enveloped by compact bone, with a center of spongy bone.
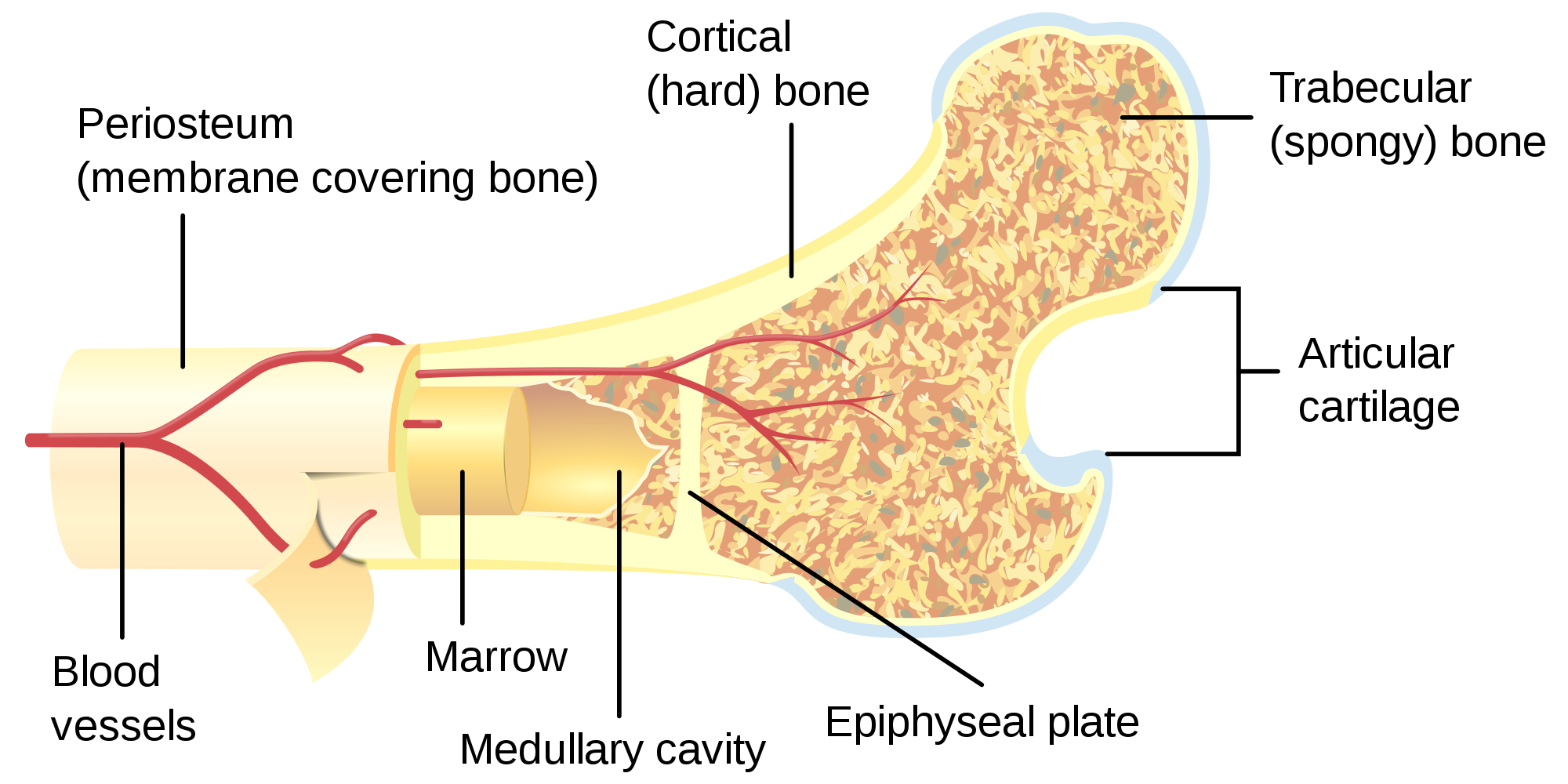
Figure 6.22Bones are more complex on the inside than you would expect from their outer appearance. This long bone has many different structural regions performing unique functions.
Figure 6.23 Flat bones are typically enveloped by compact bone, with a center of spongy bone.
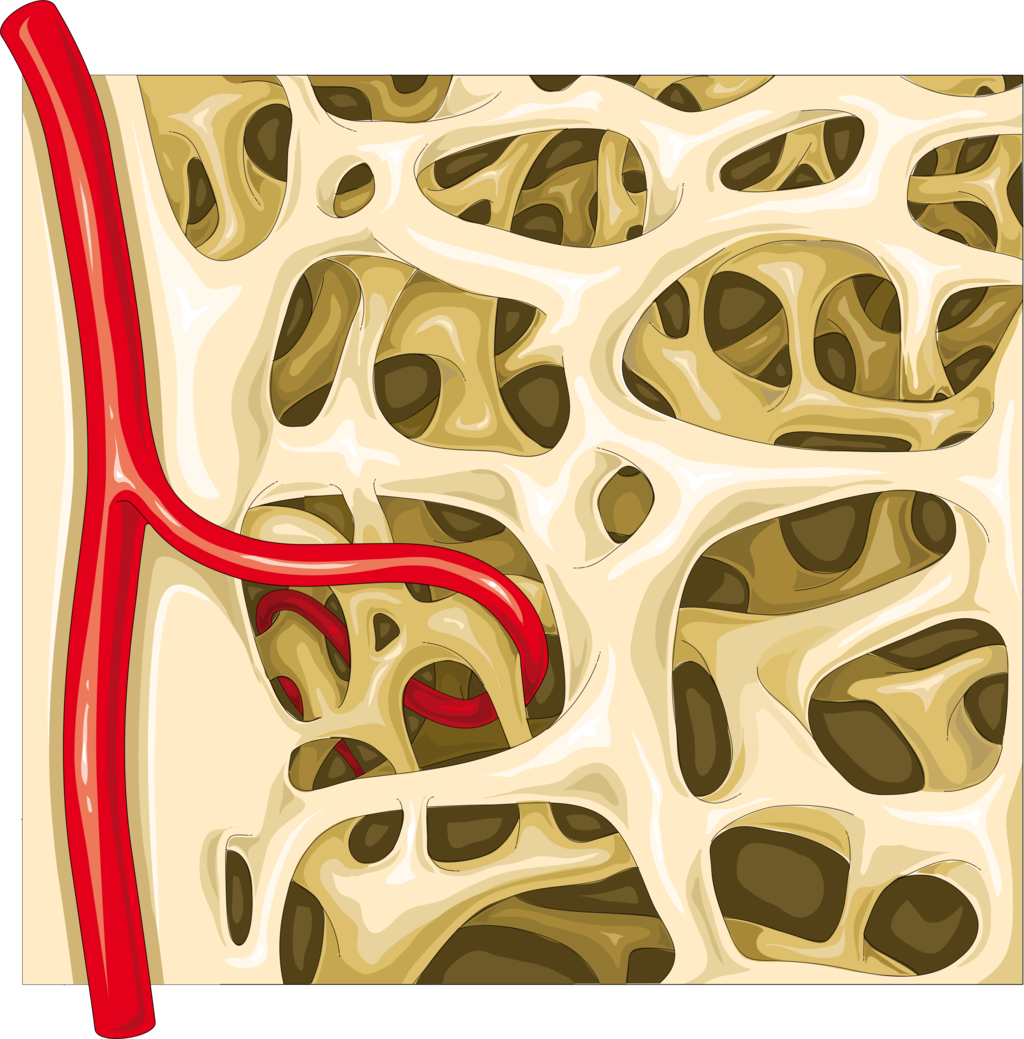
Compact bone forms the extremely hard outside layer of bones. Compact bone tissue gives bone its smooth, dense, solid appearance. It accounts for about 80% of the total bone mass of the adult skeleton. Spongy bone tissue is part or all of the interior of many bones. As its name suggests, spongy bone is porous like a sponge, containing an irregular network of spaces, as shown in Figures 6.24 and 6.25. This makes spongy bone much less dense than compact bone. Spongy bone has a greater surface area than compact bone but makes up only 20% of bone mass.
Figure 6.24Spongy bone has a lattice-like appearance. The empty spaces you can see here would be filled with bone marrow in a living person.
Figure 6.25 Spongy bone is made up of a lattice-like network of tissue and is found at the ends of long bones and in the center of many flat bones.
Both compact and spongy bone tissues have the same types of cells, but they differ in how the cells are arranged. The cells in compact bone are arranged in multiple microscopic columns, whereas the cells in spongy bone are arranged in a looser, more open network. These cellular differences explain why compact and spongy bone tissues have such different structures.
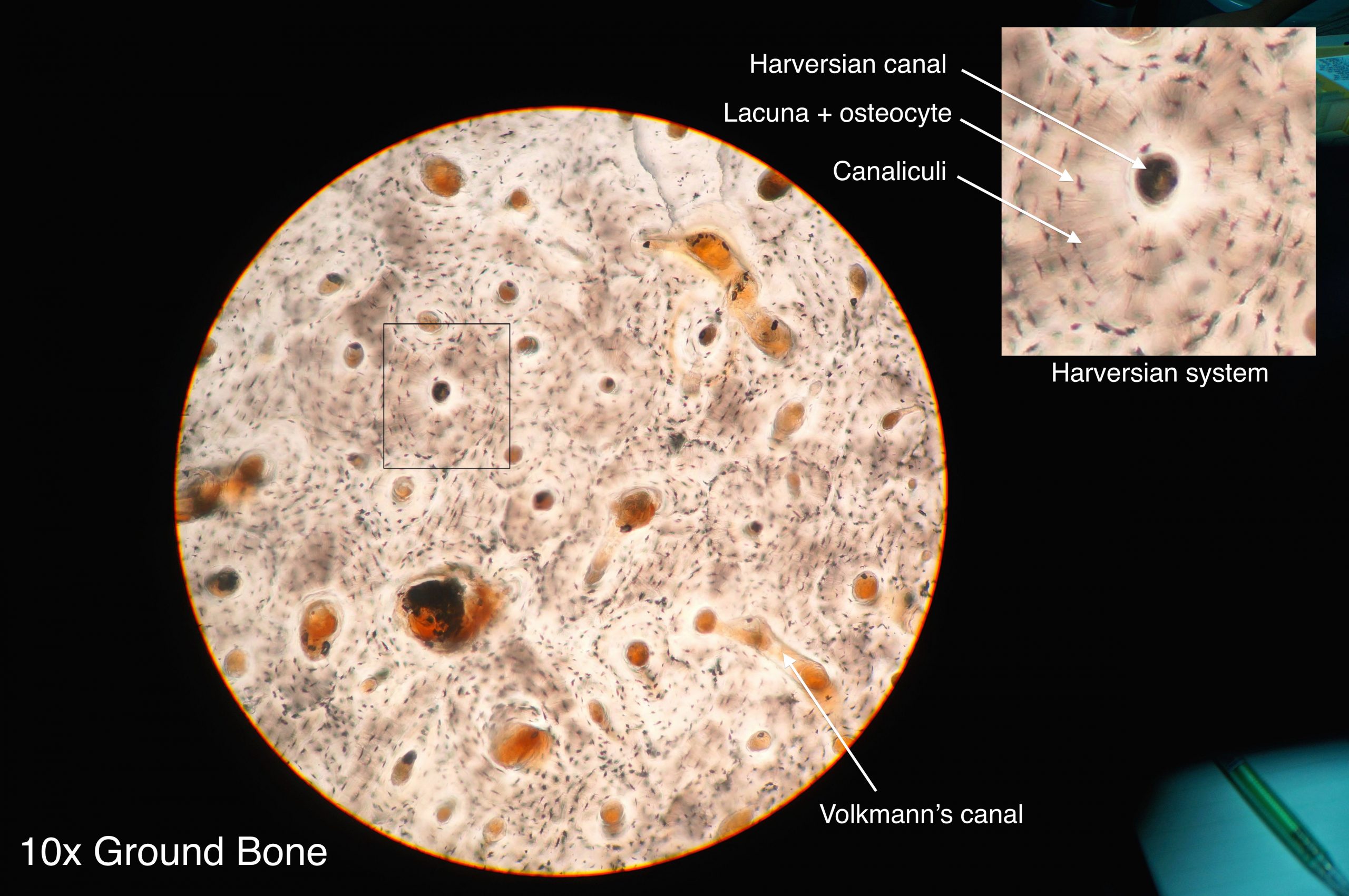
Compact bone: has a dense matrix organized into cylindrical units called osteons. Each osteon contains a central canal (sometimes called a Harversian Canal) which allows for space for blood vessels and nerves, as well as concentric rings of bone matrix and osteocytes in lacunae, as per the diagram here. Compact bone is found in long bones and forms a shell around spongy bone.
Figure 6.26 Compact bone is composed of organized units called osteons.
TISSUES IN BONES
Besides compact and spongy bone tissues, bones contain several other tissues, including blood vessels and nerves. In addition, bones contain bone marrow and periosteum.
Bone marrow is a soft connective tissue found inside a cavity, called the marrow cavity. There are two types of marrow in adults — yellow bone marrow (which consists mostly of fat) and red bone marrow. All marrow is red in newborns, but by adulthood, much of the red marrow has changed to yellow marrow. In adults, red marrow is found mainly in the femur, ribs, vertebrae, and pelvic bones. Only red bone marrow contains hematopoietic stem cells that give rise to red blood cells, white blood cells, and platelets in the process of hematopoiesis.
Periosteum is a tough, fibrous membrane that covers the outer surface of bones. It provides a protective covering for compact bone tissue. It is also the source of new bone cells.
BONE CELLS
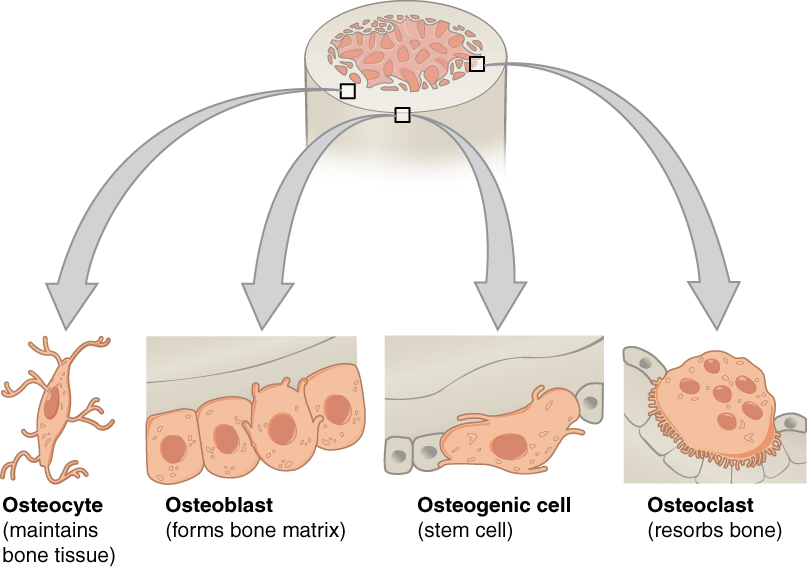
Bone tissues are composed of four different types of bone cells: osteoblasts, osteocytes, osteoclasts, and osteogenic cells.
Osteoblasts are bone cells with a single nucleus that make and mineralize bone matrix. They make a protein mixture that is composed primarily of collagen and creates the organic part of the matrix. They also release calcium and phosphate ions that form mineral crystals within the matrix. In addition, they produce hormones that play a role in the mineralization of the matrix.
Osteocytes are mainly inactive bone cells that form from osteoblasts that have become entrapped within their own bone matrix in chambers called lacunae. Osteocytes help regulate the formation and breakdown of bone tissue. They have multiple cell projections (canaliculi) that are thought to be involved in communication with other bone cells.
Osteoclasts are bone cells with multiple nuclei that resorb bone tissue and break down bone. They dissolve the minerals in bone and release them into the blood.
Osteogenic cells are undifferentiated stem cells. They are the only bone cells that can divide. When they do, they differentiate and develop into osteoblasts.
Figure 6.27 Different types of bones cells have different functions.
Bone is very active tissue. It is constantly remodeled by the work of osteoblasts and osteoclasts. Osteoblasts continuously make new bone, and osteoclasts keep breaking down bone. This allows for minor repair of bones, as well as homeostasis of mineral ions in the blood.
TYPES OF BONES
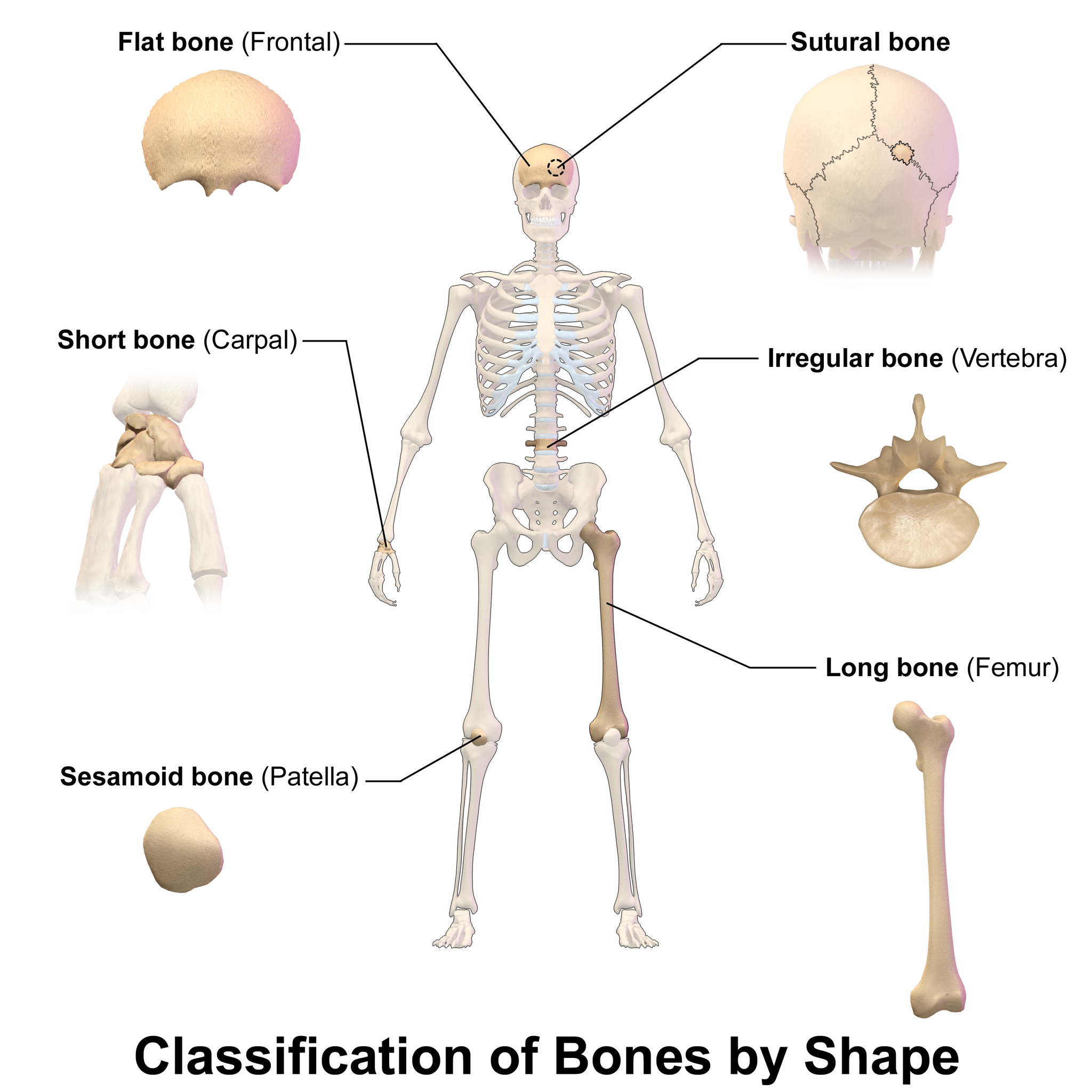
There are six types of bones in the human body, categorized based on their shape or location: long, short, flat, sesamoid, sutural, and irregular bones. You can see an example of each type of bone in Figure 6.28.
Long bones are characterized by a shaft that is much longer than it is wide, and by a rounded head at each end of the shaft. Long bones are made mostly of compact bone, with lesser amounts of spongy bone and marrow. Most bones of the limbs, including those of the fingers and toes, are long bones.
Short bones are roughly cube-shaped and have only a thin layer of compact bone surrounding a spongy bone interior. The bones of the wrists and ankles are short bones.
Flat bones are thin and generally curved, with two parallel layers of compact bone sandwiching a layer of spongy bone. Most of the bones of the skull are flat bones, as is the sternum (breastbone).
Sesamoid bones are embedded in tendons, the connective tissues that bind muscles to bones. Sesamoid bones hold tendons farther away from joints, so the angle of the tendons is increased, thus increasing the leverage of muscles. The patella (knee cap) is an example of a sesamoid bone.
Sutural bones are very small bones located between the major bones of the skull, within the joints (sutures) between the larger bones. They are not always present.
Irregular bones are those that do not fit into any of the above categories. They generally consist of thin layers of compact bone surrounding a spongy bone interior. Their shapes are irregular and complicated. Examples of irregular bones include the vertebrae and the bones of the pelvis.
Figure 6.28 This diagram shows an example of each of six types of bones classified by shape or location.
FEATURE: RELIABLE SOURCES
Diseased or damaged bone marrow can be replaced by donated bone marrow cells, which help treat and often cure many life-threatening conditions, including leukemia, lymphoma, sickle cell anemia, and thalassemia. If a bone marrow transplant is successful, the new bone marrow will start making healthy blood cells and improve the patient’s condition.
Learn more about bone marrow donation, and consider whether you might want to do it yourself. Find reliable sources to answer the following questions:
How does one become a potential bone marrow donor?
Who can and who cannot donate bone marrow?
How is a bone marrow donation made?
What risks are there in donating bone marrow?
Review
Describe osseous tissue.
Why are bones hard, but not brittle?
Compare and contrast the compact and spongy bone.
What non-osseous tissues are found in bones?
List four types of bone cells and their functions.
Identify six types of bones. Give an example of each type.
Compare and contrast yellow bone marrow and red bone marrow.
Which type of bone cell divides to produce new bone cells? Where is this cell type located?
Where do osteoblasts and osteocytes come from? How are they related to each other?
Which type of bone is embedded in tendons?
The Skeletal System: Crash Course A&P #19, CrashCourse, 2015.
6.5 BONE GROWTH, REMODELING, AND REPAIR
Figure 6.29 Water and casts don’t mix.
BREAK A LEG
Did you ever break a leg or other bone, like the man looking longingly at the water in this swimming pool (Figure 6.28)? Having a broken bone can really restrict your activity. Bones are very hard, but they will break (or fracture) if enough force is applied to them. Fortunately, bones are highly active organs that can repair themselves if they break. Bones can also remodel themselves and grow. You’ll learn how bones can do all of these things in this section.
BONE GROWTH
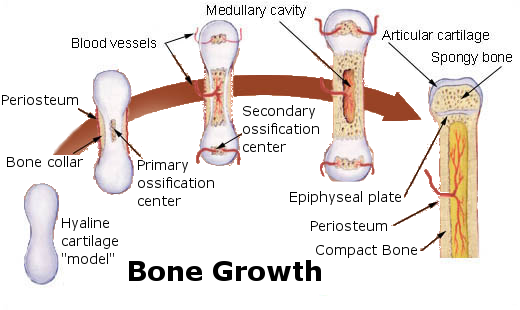
Early in the development of a human fetus, the skeleton is made almost entirely of cartilage. The relatively soft cartilage gradually turns into hard bone through ossification. Ossification is a process in which bone tissue is created from cartilage. The steps in which bones of the skeleton form from cartilage are illustrated in 6.30. The steps are as follows:
Cartilage “model” of bone forms. This model continues to grow as ossification takes place.
Ossification begins at a primary ossification center in the middle of bone.
Ossification then starts to occur at secondary ossification centers at the ends of bone.
The medullary cavity forms. This cavity will contain red bone marrow.
Areas of ossification meet at epiphyseal plates, and articular cartilage forms. Bone growth ends.
Figure 6.30 The ossification of cartilage in the human skeleton is a process that lasts throughout childhood in some bones.
The ossification of cartilage in the human skeleton is a process that lasts throughout childhood in some bones.
PRIMARY AND SECONDARY OSSIFICATION CENTERS
When bone forms from cartilage, ossification begins with a point in the cartilage called the primary ossification center. This generally appears during fetal development, although a few short bones begin their primary ossification after birth. Ossification happens toward both ends of the bone from the primary ossification center, and — in the case of long bones — it eventually forms the shaft of the bone.
Secondary ossification centers form after birth. Ossification from secondary centers eventually forms the ends of the bones. The shaft and ends of the bone are separated by a growing zone of cartilage until the individual reaches skeletal maturity.
SKELETAL MATURITY
Throughout childhood, the cartilage remaining in the skeleton keeps growing, and allows for bones to grow in size. Once all of the cartilage has been replaced by bone, and fusion has taken place at the epiphyseal plates, bones can no longer keep growing in length. At this point, skeletal maturity has been reached. It generally takes place by age 18 to 25.
The use of anabolic steroids by teens can speed up the process of skeletal maturity, resulting in a shorter period of cartilage growth before fusion takes place. This means that teens who use steroids are likely to end up shorter as adults than they would otherwise have been.
BONE REMODELING
Even after skeletal maturity has been attained, bone is constantly being resorbed and replaced with new bone in a process called bone remodeling. In this lifelong process, mature bone tissue is continually turned over, with about ten per cent of the skeletal mass of an adult being remodeled each year. Bone remodeling is carried out through the work of osteoclasts —which are bone cells that resorb bone and dissolve its minerals — and osteoblasts, which are bone cells that make new bone matrix.
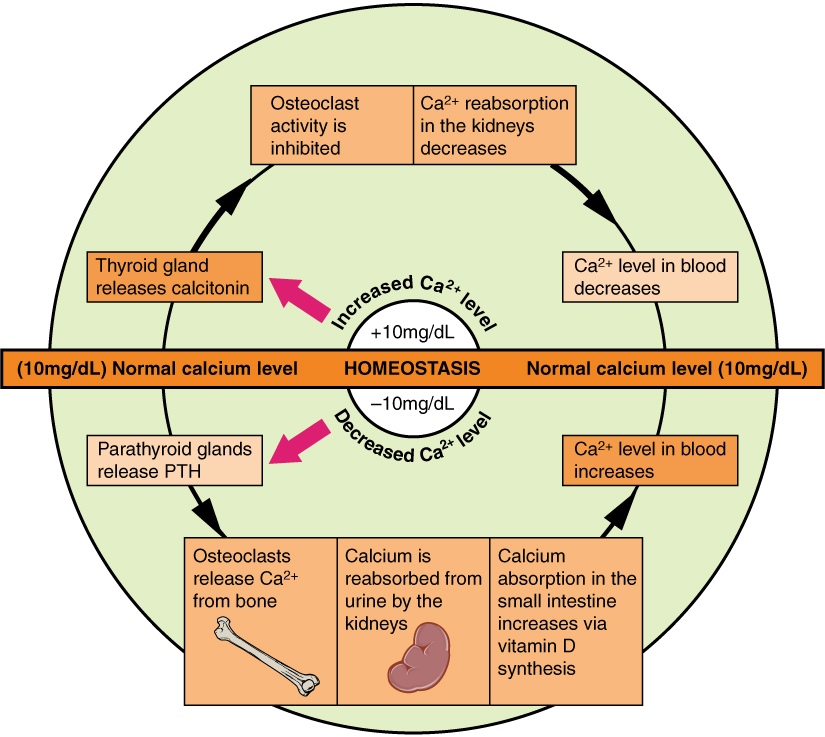
Bone remodeling serves several functions. It shapes the bones of the skeleton as a child grows, and it repairs tiny flaws in bone that result from everyday movements. Remodeling also makes bones thicker at points where muscles place the most stress on them. In addition, remodeling helps regulate mineral homeostasis, because it either releases mineral from bones into the blood or absorbs mineral from the blood into bones. Figure 6.31 shows how osteoclasts in bones are involved in calcium regulation.
Figure 6.31 Keeping the calcium level in homeostasis involves the work of osteoclasts, the bone cells that resorb bone and release calcium into the blood.
The action of osteoblasts and osteoclasts in bone remodeling and calcium homeostasis is controlled by a number of enzymes, hormones, and other substances that either promote or inhibit the activity of the cells. In this way, these substances control the rate at which bone is made, destroyed, and changed in shape. For example, the rate at which osteoclasts resorb bone and release calcium into the blood is promoted by parathyroid hormone (PTH) and inhibited by calcitonin, which is produced by the thyroid gland (see the diagram in Figure 6.31). The rate at which osteoblasts create new bone is stimulated by growth hormone, which is produced by the anterior lobe of the pituitary gland. Thyroid hormone and sex hormones (estrogens and androgens) also stimulate osteoblasts to create new bone.
Bone Remodeling and Modeling, Amgen, 2012.
BONE REPAIR
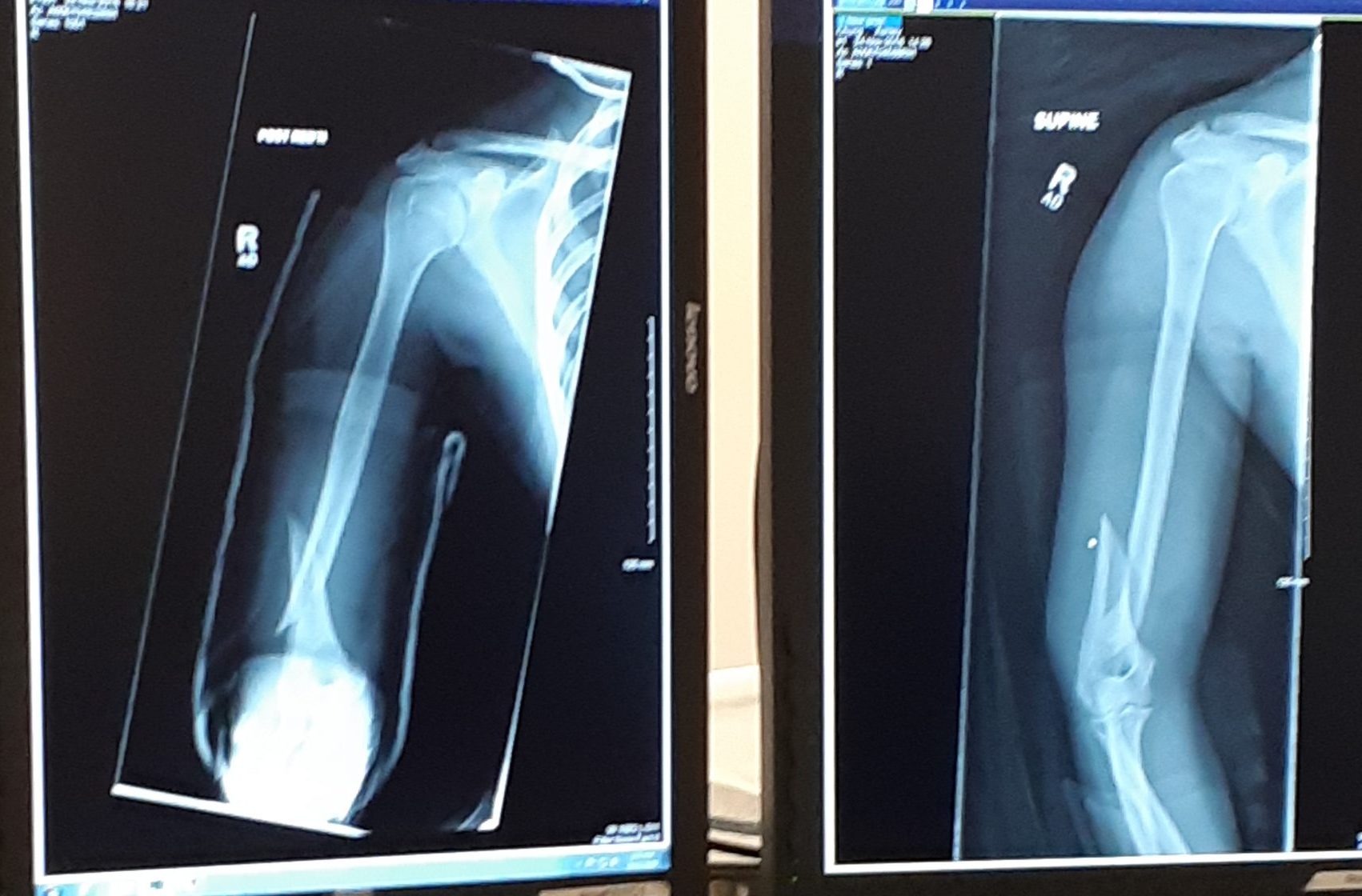
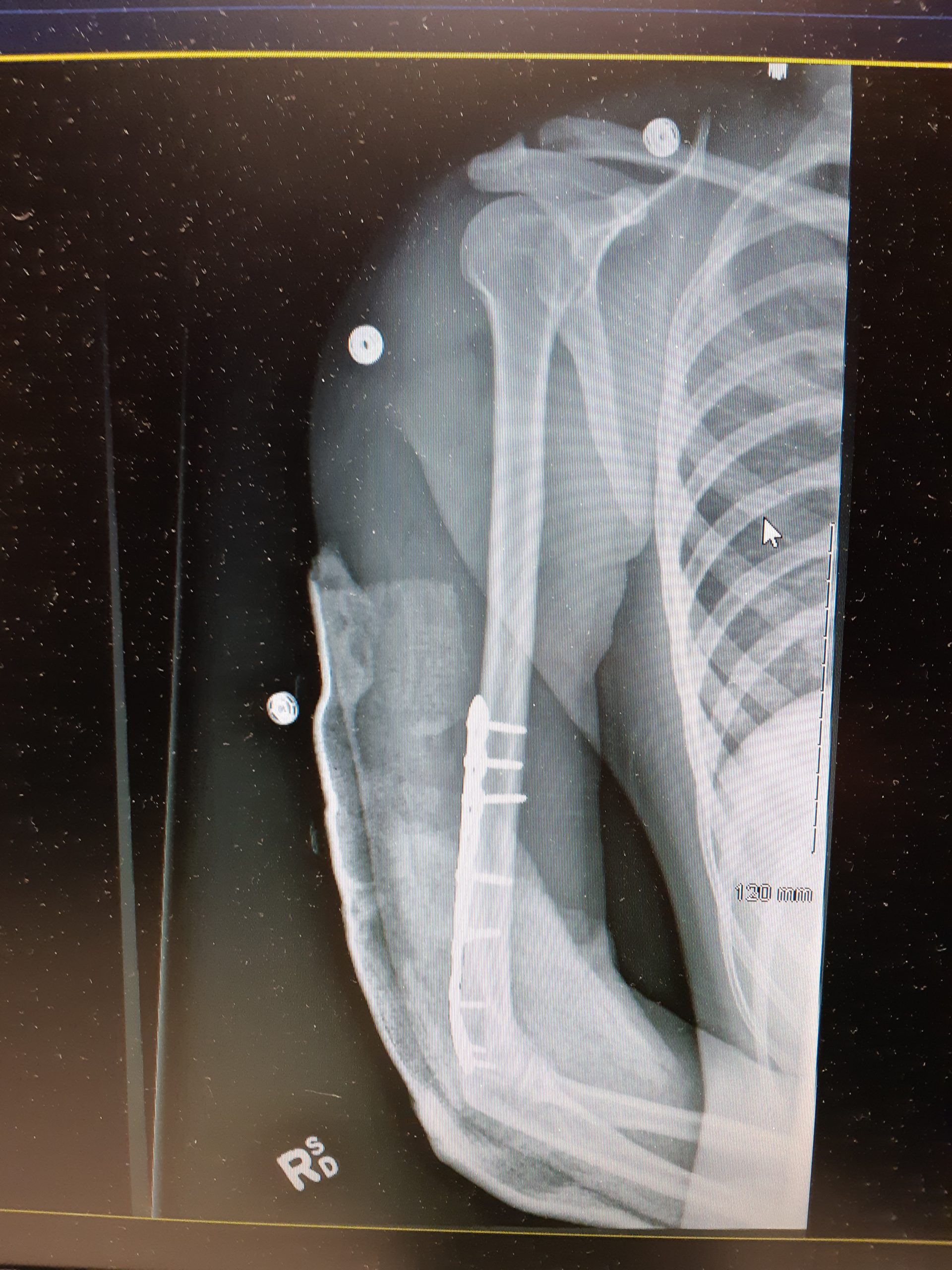
Bone repair (or healing) is the process in which a bone repairs itself following a bone fracture. You can see an X-ray of a bone fracture in Figure 6.32. In this fracture, the humerus in the upper arm has been completely broken through its shaft. Before this fracture heals, a physician must push the displaced bone parts back into their correct positions. Then, the bone must be stabilized — with a cast and/or pins surgically inserted into the bone, for example (as shown in Figure 6.33) — until the bone’s natural healing process is complete. This process may take several weeks.
Figure 6.32 A bone fracture does not always involve a complete break in the bone, as in this X-ray. Sometimes, a fracture is just a crack in the bone. In other cases, the bone not only breaks all the way through, but also breaks through the soft tissues around it so it protrudes from the skin. This is called an open fracture.
Figure 6.33 While some bones can heal by wearing a cast, others may require more invasive treatments, such as bone fracture repair. Bone fracture repair is a surgery to fix a broken bone using metal screws, pins, rods, or plates to hold the bone in place. It’s also known as open reduction and internal fixation (ORIF) surgery.
Although bone repair is a natural physiological process, it may be promoted or inhibited by several factors. Fracture repair is more likely to be successful with adequate nutrient intake. Age, bone type, drug therapy, and pre-existing bone disease are additional factors that may affect healing. Bones that are weakened by disease (such as osteoporosis or bone cancer) are not only likely to heal more slowly but are also more likely to fracture in the first place.
FEATURE: MYTH VS. REALITY
Bone fractures are fairly common, and there are many myths about them. Knowing the facts is important, because fractures generally require emergency medical treatment.
Myth
Reality
“A bone fracture is a milder injury than a broken bone.”
A bone fracture is the same thing as a broken bone.
“If you still have full range of motion in a limb, then it must not be fractured.”
Even if a bone is fractured, the muscles and tendons attached to it may still be able to move the bone normally. This is especially likely if the bone is cracked — but not broken — into two pieces. Even if a bone is broken all the way through, range of motion may not be affected if the bones on either side of the fracture remain properly aligned.
“A fracture always produces a bruise.”
Many — but not all — fractures produce a bruise. If a fracture does produce a bruise, it may take several hours (or even a day or more!) for the bruise to appear.
“Fractures are so painful that you will immediately know if you break a bone.”
Ligament sprains and muscle strains are also very painful, sometimes more painful than fractures. Additionally, every person has a different pain tolerance. People with a high pain tolerance may continue using a broken bone in spite of the pain.
“You can tell when a bone is fractured because there will be very localized pain over the break.”
A broken bone is often accompanied by injuries to surrounding muscles or ligaments. As a result, the pain may extend far beyond the location of the fracture. The pain may be greater directly over the fracture, but the intensity of the pain may make it difficult to pinpoint exactly where the pain originates.
Review
Outline how bone develops starting early in the fetal stage, and through the age of skeletal maturity.
Describe the process of bone remodeling. When does it occur?
What purposes does bone remodeling serve?
Define bone repair. How long does this process take?
Explain how bone repair occurs.
Identify factors that may affect bone repair.
When calcium levels are low, which type of bone cell causes the release of calcium to the bloodstream?
Which tissue and bone cell type are primarily involved in bone repair after a fracture?
Healing Process of Bone Fracture, Aldo Fransiskus Marsetio, 2015.
6.6 JOINTS
Figure 6.34 That’s quite a stretch!
DOUBLE JOINTED?
Is this woman double jointed? No, there is actually no such thing — at least as far as humans are concerned. However, some people, like the woman pictured in Figure 11.6.1, are much more flexible than others, generally because they have looser ligaments. Physicians call this condition joint hypermobility. Regardless of what it’s called, the feats of people with highly mobile joints can be quite impressive.
WHAT ARE JOINTS?
Joints are locations at which bones of the skeleton connect with one another. A joint is also called an articulation. The majority of joints are structured in such a way that they allow movement. However, not all joints allow movement. Of joints that do allow movement, the extent and direction of the movements they allow also vary.
CLASSIFICATION OF JOINTS
Joints can be classified structurally or functionally. The structural classification of joints depends on the manner in which the bones connect to each other. The functional classification of joints depends on the nature of the movement the joints allow. There is significant overlap between the two types of classifications, because function depends largely on structure.
STRUCTURAL CLASSIFICATION OF JOINTS
The structural classification of joints is based on the type of tissue that binds the bones to each other at the joint. There are three types of joints in the structural classification: fibrous, cartilaginous, and synovial joints.
Fibrous joints are joints in which bones are joined by dense connective tissue that is rich in collagen fibres. These joints are also called sutures. The joints between bones of the cranium are fibrous joints.
Cartilaginous joints are joints in which bones are joined by cartilage. The joints between most of the vertebrae in the spine are cartilaginous joints.
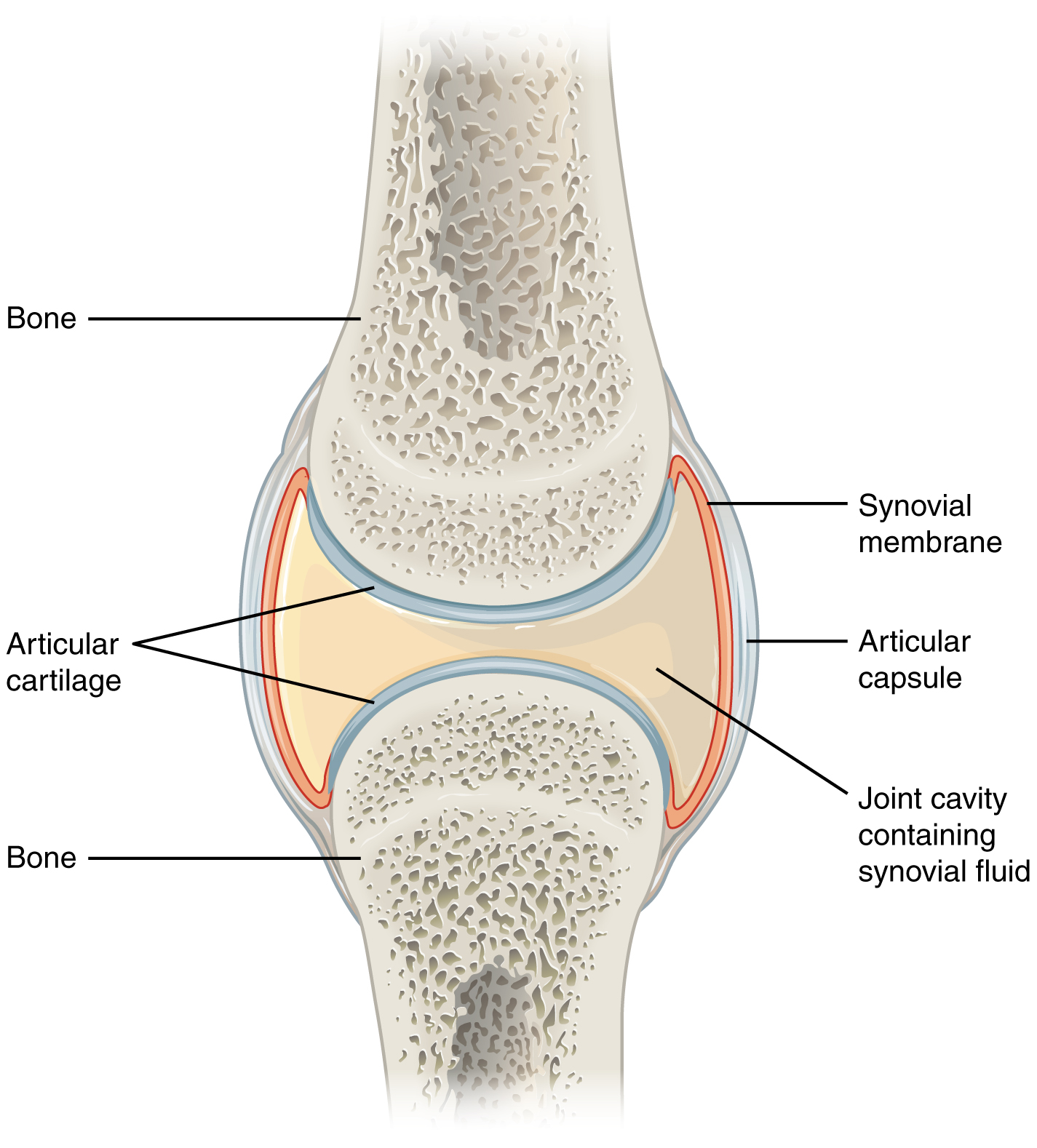
Synovial joints are characterized by a fluid-filled space (called a synovial cavity) between the bones of the joints. You can see a drawing of a typical synovial joint in Figure 6.35. The cavity is enclosed by a membrane and filled with a fluid (called synovial fluid) that provides extra cushioning to the ends of the bones. Cartilage covers the articulating surfaces of the two bones, but the bones are actually held together by ligaments. The knee is a synovial joint.
Figure 6.35 A typical synovial joint is represented by this diagram.
FUNCTIONAL CLASSIFICATION OF JOINTS
The functional classification of joints is based on the type and degree of movement that they allow. There are three types of joints in the functional classification: immovable, partly movable, and movable joints.
Immovable joints allow little or no movement at the joint. Most immovable joints are fibrous joints. Besides the bones of the cranium, immovable joints include joints between the tibia and fibula in the lower leg, and between the radius and ulna in the lower arm.
Partly movable joints permit slight movement. Most partly movable joints are cartilaginous joints. Besides the joints between vertebrae, they include the joints between the ribs and sternum (breastbone).
Movable joints allow bones to move freely. All movable joints are synovial joints. Besides the knee, they include the shoulder, hip, and elbow. Movable joints are the most common type of joints in the body. Movable joints can be classified further according to the type of movement they allow. In this chapter, we will focus on two of these: hinge and ball-and-socket joints. A ball-and-socket joint allows the greatest range of movement of any movable joint. It allows forward and backward motion, as well as upward and downward movement. It also allows rotation in a circle. The hip and shoulder are the only two ball-and-socket joints in the human body. A hinge joint allows back and forth movement like the hinge of a door. An example of a hinge joint is the elbow. This joint allows the arm to bend back and forth.
Review
What are joints?
What are two ways that joints are commonly classified?
How are joints classified structurally?
Describe the functional classification of joints.
How are movable joints classified?
Name the two types of movable joints. Describe how they move and give an example of each.
Which specific type of moveable joint do you think your knee joint is? Explain your reasoning.
Explain the difference between cartilage in a cartilaginous joint and cartilage in a synovial joint.
Why are fibrous joints immovable?
What is the function of synovial fluid?
6.7 DISORDERS OF THE SKELETAL SYSTEM
COMMON SKELETAL SYSTEM DISORDERS
A number of disorders affect the skeletal system, including bone fractures and bone cancers. However, the two most common disorders of the skeletal system are osteoporosis and osteoarthritis. At least ten million people in the United States have osteoporosis, and more than eight million of them are women. Osteoarthritis is even more common, affecting almost 1.4 million people in Canada, and 1 in 4 women over the age of 50. Because osteoporosis and osteoarthritis are so common, they are the focus of this section. These two disorders are also good examples to illustrate the structure and function of the skeletal system.
OSTEOPOROSIS
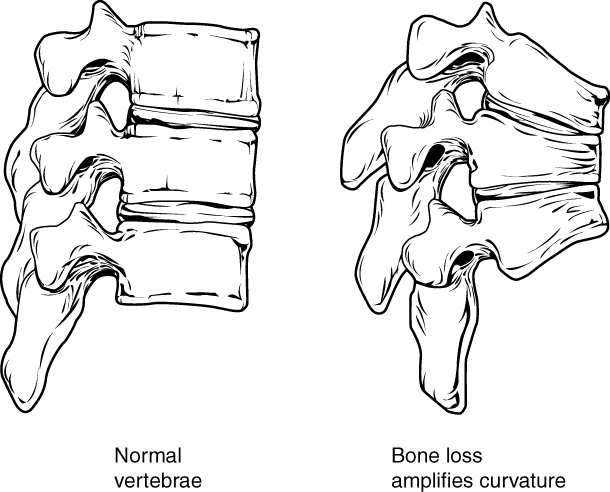
Osteoporosis is an age-related disorder in which bones lose mass, weaken, and break more easily than normal bones. Bones may weaken so much that a fracture can occur with minor stress — or even spontaneously, without any stress at all. Osteoporosis is the most common cause of broken bones in the elderly, but until a bone fracture occurs, it typically causes no symptoms. The bones that break most often include those in the wrist, hip, shoulder, and spine. When the thoracic vertebrae are affected, there can be a gradual collapse of the vertebrae due to compression fractures, as shown in Figure 11.7.2. This is what causes kyphosis, as pictured above in Figure 6.36.
Figure 6.36 Compression fractures of thoracic vertebrae are relatively common in people with osteoporosis.
CHANGES IN BONE MASS WITH AGE
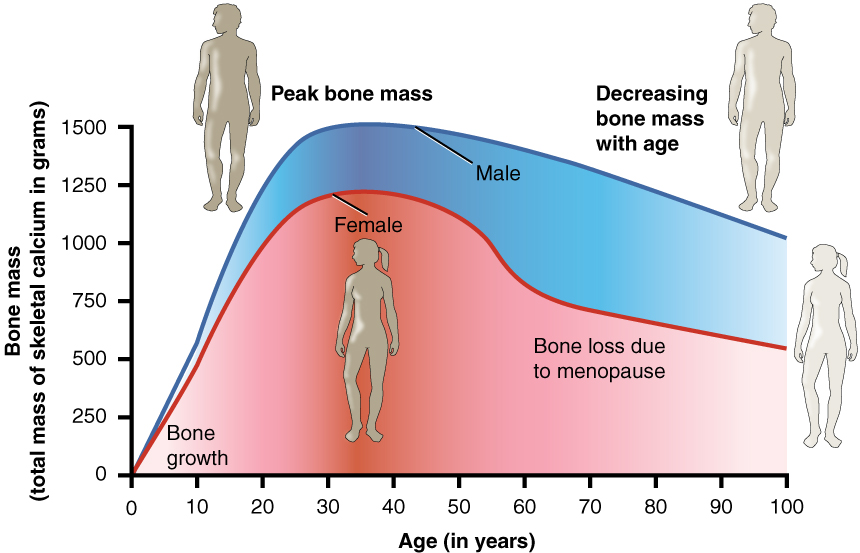
As shown in the Figure 6.37, bone mass in both males and females generally peaks when people are in their thirties, with males typically attaining a higher peak mass than females. In both sexes, bone mass usually decreases after that, and this tends to occur more rapidly in females, especially after menopause. The greater decrease in females is generally attributable to low levels of estrogen in the post-menopausal years.
Figure 6.37 Bone mass is a measure of the total mass of calcium in the bones of the skeleton. As bone mass decreases, the risk of fractures increases.
WHAT CAUSES OSTEOPOROSIS?
The underlying mechanism in all cases of osteoporosis is an imbalance between bone formation by osteoblasts and bone resorption by osteoclasts. Normally, bones are constantly being remodeled by these two processes, with up to ten per cent of all bone mass undergoing remodeling at any point in time. As long as these two processes are in balance, no net loss of bone occurs. There are three main ways that an imbalance between bone formation and bone resorption can occur and lead to a net loss of bone. All three ways may occur in the same individual. The three ways are described below:
An individual never develops normal peak bone mass during the young adult years: If the peak level is lower than normal, then there is less bone mass to begin with, making osteoporosis more likely to develop.
There is greater than normal bone resorption: Bone resorption normally increases after peak bone mass is reached, but age-related bone resorption may be greater than normal for a variety of reasons. One possible reason is calcium or vitamin D deficiency, which causes the parathyroid gland to release PTH, the hormone that promotes resorption by osteoclasts.
There is inadequate formation of new bone by osteoblasts during remodeling: Lack of estrogen may decrease the normal deposition of new bone. Inadequate levels of calcium and vitamin D also lead to impaired bone formation by osteoblasts.
An imbalance between bone building and bone destruction leading to bone loss may also occur as a side effect of other disorders. For example, people with alcoholism, anorexia nervosa, or hyperthyroidism have an increased rate of bone loss. Some medications — including anti-seizure medications, chemotherapy drugs, steroid medications, and some antidepressants — also increase the rate of bone loss.
DIAGNOSING OSTEOPOROSIS
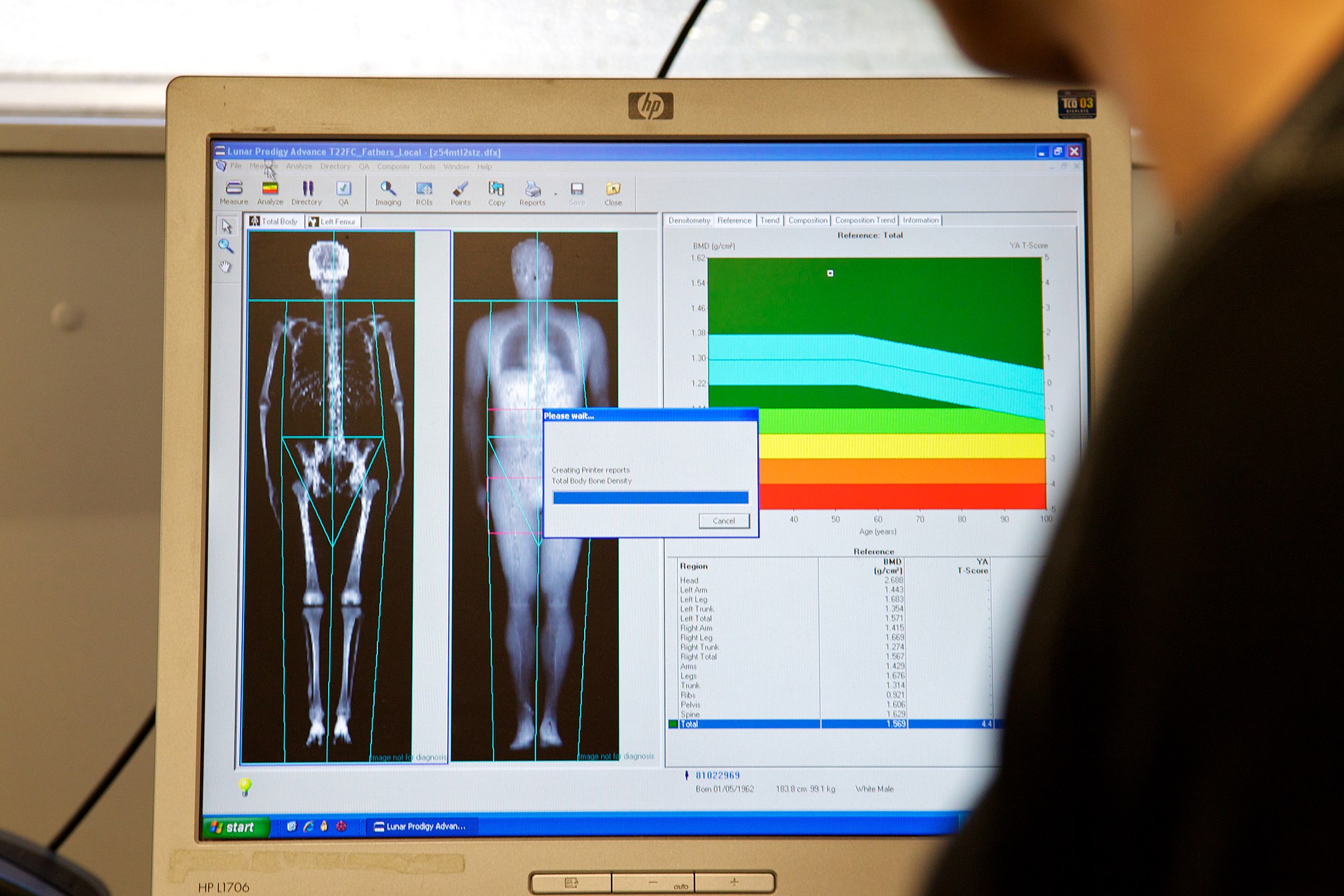
Osteoporosis is diagnosed by measuring a patient’s bone density and comparing it with the normal level of peak bone density in a young adult reference population of the same sex as the patient. If the patient’s bone density is too far below the normal peak level (as measured by a statistic called a T-score), then osteoporosis is diagnosed. Bone density is usually measured by a type of X-ray called dual-energy X-ray absorptiometry (or DEXA), an example of which is shown in Figure 6.38. Typically, the density is measured at the hip. Sometimes, other areas are also measured, because there may be variation in bone density in different parts of the skeleton. Osteoporosis Canada recommends that all women 65 years of age and older be screened with DEXA for bone density. Screening may be recommended at younger ages in people with risk factors for osteoporosis (see Risk Factors for Osteoporosis below).
Figure 6.38 Dual-energy X-ray absorptiometry is a means of measuring bone mineral density using spectral imaging. Two X-ray beams, with different energy levels, are aimed at the patient’s bones. When soft tissue absorption is subtracted out, the bone mineral density can be determined from the absorption of each beam by bone.
OSTEOPOROTIC FRACTURES
Fractures are the most dangerous aspect of osteoporosis, and osteoporosis is responsible for millions of fractures annually. Debilitating pain among the elderly is often caused by fractures from osteoporosis, and it can lead to further disability and early mortality. Fractures of the long bones (such as the femur) can impair mobility and may require surgery. Hip fracture usually requires immediate surgery, as well. The immobility associated with fractures — especially of the hip — increases the risk of deep vein thrombosis, pulmonary embolism, and pneumonia. Osteoporosis is rarely fatal, but these complications of fractures often are. Older people tend to have more falls than younger people, due to such factors as poor eyesight and balance problems, increasing their risk of fractures even more. The likelihood of falls can be reduced by removing obstacles and loose carpets or rugs in the living environment.
RISK FACTORS FOR OSTEOPOROSIS
There are a number of factors that increase the risk of osteoporosis. Eleven of them are listed below. The first five factors cannot be controlled, but the remaining factors generally can be controlled by changing behaviors.
Older age
Female sex
European or Asian ancestry
Family history of osteoporosis
Short stature and small bones
Smoking
Alcohol consumption
Lack of exercise
Vitamin D deficiency
Poor nutrition
Consumption of soft drinks
TREATMENT AND PREVENTION OF OSTEOPOROSIS
Osteoporosis is often treated with medications that may slow or even reverse bone loss. Medications called bisphosphonates, for example, are commonly prescribed. Bisphosphonates slow down the breakdown of bone, allowing bone rebuilding during remodeling to keep pace. This helps maintain bone density and decreases the risk of fractures. The medications may be more effective in patients who have already broken bones than in those who have not, significantly reducing their risk of another fracture. Generally, patients are not recommended to stay on bisphosphonates for more than three or four years. There is no evidence for continued benefit after this time — in fact, there is a potential for adverse side effects.
Figure 6.39 Hiking is an enjoyable way to help keep bones strong and reduce the risk of osteoporosis.
Preventing osteoporosis includes eliminating any risk factors that can be controlled through changes of behavior. If you smoke, stop. If you drink, reduce your alcohol consumption — or cut it out altogether. Eat a nutritious diet and make sure you are getting adequate amounts of vitamin D. You should also avoid drinking carbonated beverages.
If you’re a couch potato, get involved in regular exercise. Aerobic, weight-bearing, and resistance exercises can all help maintain or increase bone mineral density (for example hiking as in Figure 6.39). Exercise puts stress on bones, which stimulates bone building. Good weight-bearing exercises for bone building include weight training, dancing, stair climbing, running, and hiking (see Figure 11.7.5). Biking and swimming are less beneficial, because they don’t stress the bones. Ideally, you should exercise for at least 30 minutes a day most days of the week.
Osteoarthritis
Figure 6.40 The areas shaded in blue indicate the joints most commonly affected by OA.
Osteoarthritis (OA) is a joint disease that results from the breakdown of joint cartilage and bone. The most common symptoms are joint pain and stiffness. Other symptoms may include joint swelling and decreased range of motion. Initially, symptoms may occur only after exercise or prolonged activity, but over time, they may become constant, negatively affecting work and normal daily activities. As shown in Figure 6.40, the most commonly involved joints are those near the ends of the fingers, at the bases of the thumbs, and in the neck, lower back, hips, and knees. Often, joints on one side of the body are affected more than those on the other side.
WHAT CAUSES OSTEOARTHRITIS?
OA is thought to be caused by mechanical stress on the joints with insufficient self-repair of cartilage. The stress may be exacerbated by low-grade inflammation of the joints, as cells lining the joint attempt to remove breakdown products from cartilage in the synovial space. OA develops over decades as stress and inflammation cause increasing loss of articular cartilage. Eventually, bones may have no cartilage to separate them, so bones rub against one another at joints. This damages the articular surfaces of the bones and contributes to the pain and other symptoms of OA. Because of the pain, movement may be curtailed, leading to loss of muscle, as well.
DIAGNOSING OSTEOARTHRITIS
Figure 6.41 A bunion is a common sign of osteoarthritis. It is typically located at the base of the big toe.
Diagnosis of OA is typically made on the basis of signs and symptoms. Signs include joint deformities, such as bony nodules on the finger joints or bunions on the feet (as illustrated in Figure 6.41). Symptoms include joint pain and stiffness. The pain is usually described as a sharp ache or burning sensation, which may be in the muscles and tendons around the affected joints, as well as in the joints themselves. The pain is usually made worse by prolonged activity, and it typically improves with rest. Stiffness is most common when first arising in the morning, and it usually improves quickly as daily activities are undertaken.
X-rays or other tests are sometimes used to either support the diagnosis of OA or to rule out other disorders. Blood tests might be done, for example, to look for factors that indicate rheumatoid arthritis (RA), an autoimmune disease in which the immune system attacks the body’s joints. If these factors are not present in the blood, then RA is unlikely, and a diagnosis of OA is more likely to be correct.
RISK FACTORS FOR OSTEOARTHRITIS
Age is the chief risk factor for osteoarthritis. By age 65, as many as 80 per cent of all people have evidence of osteoarthritis. However, people are more likely to develop OA — especially at younger ages — if they have had a joint injury. A high school football player might have a bad knee injury that damages the joint, leading to OA in the knee by the time he is in his thirties. If people have joints that are misaligned due to congenital malformations or disease, they are also more likely to develop OA. Excess body weight is another factor that increases the risk of OA, because of the added stress it places on weight-bearing joints.
Researchers have found that people with a family history of OA have a heightened risk of developing the disorder, which suggests that genetic factors are also involved in OA. It is likely that many different genes are needed for normal cartilage and cartilage repair. If such genes are defective and cartilage is abnormal or not normally repaired, OA is more likely to result.
TREATMENT AND PREVENTION OF OSTEOARTHRITIS
OA cannot be cured, but the symptoms — especially the pain — can often be treated successfully to maintain good quality of life for people with OA. Treatments include exercise, efforts to decrease stress on joints, pain medications, and surgery.
Exercise
Exercise helps maintain joint mobility and also increases muscle strength. Stronger muscles may help keep the bones in joints correctly aligned, and this can reduce joint stress. Good exercises for OA include swimming, water aerobics (see Figure 6.42 below), and biking. These activities are recommended for OA, because they put relatively little stress on the joints.
Figure 6.42 Exercising in water provides buoyancy that places less stress on joints than the same exercises would on the ground or other hard surface.
Exercising in water provides buoyancy that places less stress on joints than the same exercises would on the ground or other hard surface.
De-stressing Joints
Efforts to decrease stress on joints include resting and using mobility devices such as canes, which reduce the weight placed on weight-bearing joints and also improve stability. In people who are overweight, losing weight may also reduce joint stress.
Pain Medications
The first type of pain medication likely to be prescribed for OA is acetaminophen (e.g., Tylenol). When taken as prescribed, it has a relatively low risk of serious side effects. If this medication is inadequate to relieve the pain, non-steroidal anti-inflammatory drugs (NSAIDs, such as ibuprofen) may be prescribed. NSAIDs, however, are more likely to cause serious side effects, such as gastrointestinal bleeding, elevated blood pressure, and increased risk of stroke. Opioids usually are reserved for patients who have suffered serious side effects or for whom other medications have failed to relieve pain. Due to the risk of addiction, only short-term use of opioids is generally recommended.
Surgery
Joint-replacement surgery is the most common treatment for serious OA in the knee or hip. In fact, knee and hip replacement surgeries are among the most common of all surgeries. Although they require a long period of healing and physical rehabilitation, the results are usually worth it. The replacement “parts” are usually pain-free and fully functional for at least a couple of decades. Quality, durability, and customization of artificial joints are constantly improving.
Prevention
If you protect your joints, you can reduce your chances of joint damage, pain, and disability. If you already have joint damage, it is equally important to protect your joints and limit further damage. Follow these five tips:
Maintain a normal, healthyweight. The more you weigh, the more force you exert on your joints. When you walk, each knee has to bear a force equal to as much as six times your body weight. If a person weighs 200 pounds, each knee bears more than half a ton of weight with every step. Seven in ten knee replacement surgeries for osteoarthritis can be attributed to obesity.
Avoid too much high-impactexercise. Examples of high-impact activities include volleyball, basketball, and tennis. These activities generally involve running or jumping on hard surfaces, which puts tremendous stress on weight-bearing joints, especially the knees. Replace some or all of your high-impact activities with low-impact activities, such as biking, swimming, yoga, or lifting light weights.
Reduce your risk of injury. Don’t be a weekend warrior, sitting at a desk all week and then crowding all your physical activity into two days. Get involved in a regular, daily exercise routine that keeps your body fit and your muscles toned. Building up muscles will make your joints more stable, allowing stress to spread across them. Be sure to do some stretching every day to keep the muscles around joints flexible and less prone to injury.
Distribute work over your body, and use your largest, strongest joints. Use your shoulder, elbow, and wrist to lift heavy objects — not just your fingers. Hold small items in the palm of your hand, rather than by the fingers. Carry heavy items in a backpack, rather than in your hands. Hold weighty objects close to your body, instead of at arms’ length. Lift with your hips and knees, not your back.
Respect pain. If it hurts, stop doing it. Take a break from the activity — at least until the pain stops. Try to use joints only to the point of mild fatigue, not pain.
Feature: Myth vs. Reality
About one out of every 5 adults in Canada suffer from osteoarthritis. The more you know about this disease, the more you can do to avoid it or slow its progression. That means knowing the facts, rather than believing the myths about osteoarthritis.
MYTH
REALITY
“Cracking my knuckles will cause osteoarthritis.”
Cracking your knuckles may lead to inflammation of your tendons, but it will not cause osteoarthritis.
“My diet has no effect on my joints.”
What and how much you eat does affect your body weight, and every pound you gain translates into an additional four pounds (or more!) of stress on your knees. Being overweight, therefore, increases the chances of developing osteoarthritis — and also the rate at which it progresses.
“Exercise causes osteoarthritis or makes it worse, so I should avoid it.”
This is one of the biggest myths about osteoarthritis. Low-impact exercise can actually lessen the pain and improve other symptoms of osteoarthritis. If you don’t have osteoarthritis, exercise can reduce your risk of developing it. Low-impact exercise helps keep the muscles around joints strong and flexible, so they can help stabilize and protect the joints.
“If my mom or dad has osteoarthritis, I will also develop it.”
It is true that you are more likely to develop osteoarthritis if a parent has it, but it isn’t a sure thing. There are several things you can do to decrease your risk, such as getting regular exercise and maintaining a healthy weight.
“Bad weather causes osteoarthritis.”
Weather conditions do not cause osteoarthritis, although in some people who already have osteoarthritis, bad weather seems to make the symptoms worse. It is primarily low barometric pressure that increases osteoarthritis pain, probably because it leads to greater pressure inside the joints relative to the outside air pressure. Some people think their osteoarthritis pain is worse in cold weather, but systematic studies have not found convincing evidence for this.
“Joint pain is unavoidable as you get older, so there is no need to see a doctor for it.”
Many people with osteoarthritis think there is nothing that can be done for the pain of osteoarthritis, or that surgery is the only treatment option. In reality, osteoarthritis symptoms often can be improved with a combination of exercise, weight loss, pain management techniques, and pain medications. If osteoarthritis pain interferes with daily life and lasts more than a few days, you should see your doctor.
“Osteoarthritis is inevitable in seniors.”
Although many people over 65 develop osteoarthritis, there are many people who never develop it, no matter how old they live to be. You can reduce your risk of developing osteoarthritis in later life by protecting your joints throughout life.
Review
Create a brochure or poster about osteoporosis to educate others about this disease. Include information about:
A definition of osteoporosis
Causes
Dangers of living with the disease
Canadian osteoporosis statistics
Risk factors
Diagnosis
Treatment
Why is it important to build sufficient bone mass in your young adult years?
Explain the difference in cause between rheumatoid arthritis and osteoarthritis.
Debunk the myth: Osteoarthritis is caused by physical activity, so people who are equally active are equally susceptible to it.
Explain how we know that estrogen generally promotes production of new bone.
Kevin Stone: The bio-future of joint replacement, TED, 2010.
CASE STUDY: A PAIN IN THE FOOT
Sophia loves wearing high heels when she goes out at night. She knows they are not the most practical shoes, but she likes how they look.
Lately, she has been experiencing pain in the balls of her feet — the area just behind the toes. Even when she trades her heels for comfortable sneakers, it still hurts when she stands or walks.
What could be going on? She searches online to try to find some answers. She finds a reputable source for foot pain information — a website from a professional organization of physicians that peer reviews the content by experts in the field. There, she reads about a condition called metatarsalgia, which produces pain in the ball of the foot that sounds very similar to what she is experiencing.
She learns that a common cause of metatarsalgia is the wearing of high heels. Shoes like this push the foot into an abnormal position, resulting in excessive pressure being placed on the ball of the foot. Looking at the photograph above (Figure 11.1.1), you can imagine how much of the woman’s body weight is focused on the ball of her foot, because of the shape of her high heels. If she were not wearing high heels, her weight would be more evenly distributed across her foot.
As she reads more about the hazards of high heels, Sophia learns that they can also cause foot deformities, such as hammertoes, bunions, and small cracks in bone called stress fractures. High heels may even contribute to the development of osteoarthritis of the knees at an early age.
Think about the following questions:
Sophia suspects she has a condition called metatarsalgia. This term is related to the term “metatarsals.” What are metatarsals, where are they located, and how do you think they are related to metatarsalgia?
High heels can cause stress fractures, which are small cracks in bone that usually appear after repeated mechanical stress, instead of after a significant acute injury. What other condition described in this chapter involves a similar process?
What are bunions and osteoarthritis of the knee? Why do you think they can be caused by wearing high heels?
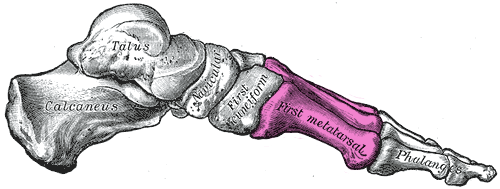
As Sophia discovered in the beginning of the chapter, wearing high heels can result in a condition called metatarsalgia. Metatarsalgia is named for the metatarsal bones, which are the five bones that run through the ball of the foot just behind the toes (highlighted in Figures 6.43 and 6.44). Wearing high heels causes excessive pressure on the ball of the foot, as described in the beginning of this chapter. Additionally, the toes are forced to pull upward in high heels, which moves the fleshy padding away from the ball of the foot and adds to the overall pressure placed on this region. Over time, this can cause inflammation and direct stress on the bones, resulting in the pain in the ball of the foot known as metatarsalgia. The pain occurs especially in weight-bearing positions, such as standing, walking, or running — which is what Sophia was experiencing. There may also be pain, numbness, or tingling in the toes associated with metatarsalgia.
Figure 6.43Metatarsalgia is a painful and even debilitating condition characterized by pain in the ball of your foot with worsens when you stand, run, walk or flex your foot.
Figure 6.44Illustration of the bones of the foot, with the metatarsal bones highlighted in pink.
Wearing high heels can also cause stress fractures in the feet, which are tiny breaks in bone that occur due to repeated mechanical stress. This is caused by the excessive pressure that high heels put on some of the bones of the feet. These fractures are somewhat similar to what occurs in osteoporosiswhen the bone mass decreases to the point where bones can fracture easily as a person goes about their daily activities. In both cases, a major noticeable injury is not necessary to create the tiny fractures.
Don’t think you are immune to stress fractures just because you don’t wear high heels! This injury also commonly occurs in people who participate in sports involving repetitive striking of the foot on the ground, such as running, tennis, basketball, or gymnastics. They may be avoided by taking preventative measures. You should ramp up any increase in activity slowly, cross-train by engaging in a variety of different sports or activities, rest if you experience pain, and wear well-cushioned and supportive running shoes. It is important to know that your cardiovascular and muscular systems adapt to an increase in physical activity much more quickly than the skeletal system.
Sophia learned through her online research that wearing high heels can also lead to foot deformities, such as bunions and hammertoes. As you learned in an earlier chapter, a bunion is a protrusion on the side of the foot, most often at the base of the big toe. It can be caused by wearing shoes with a narrow, pointed toe box — a common shape for high heels. The pressure of the shoes on the side of the foot causes an enlargement of bone or inflammation of other tissues in the region, which pushes the big toe toward the other toes.
Hammertoes are an abnormal bend in the middle joint of the second, third, or fourth toe (with the big toe being the first toe), causing the toe to be shaped similarly to a hammer. The narrow, pointed toe box of many high heels, combined with the way the toes are squished into the front of the shoe as a result of the height of the heel, can cause the toes to become deformed this way. Treatments for bunions and hammertoe include wearing shoes with a roomy toe box, padding or taping the toes, and toe exercises and stretches. If the bunion or hammertoe does not respond to these treatments, surgery may be necessary to correct the deformity.
Because the bones of the skeleton are connected and work together with other systems to support the body, wearing high heels can also cause physical problems in areas other than the feet. Wearing high heels shifts a person’s posture and alignment, and can put strain on tendons, muscles, and other joints in the body. Research published in 2014 from a team at Stanford University suggests that wearing high heels, particularly if the person is overweight or the heels are very high, may increase the risk of osteoarthritis (OA) in the knee, due to added stress on the knee joint as the person walks. As you have learned, OA results from the breakdown of cartilage and bone at the joint. Because it can only be treated to minimize symptoms — and not for a cure — OA could be an unfortunate long-term consequence of wearing high heels.
Sophia has decided that wearing high heels regularly is not worth the pain and potential long-term damage to her body. After consulting with her doctor, who confirmed she had metatarsalgia, she was able to successfully treat it with ice, rest, and wearing comfortable, supportive shoes instead of heels.
High heels are not the only kind of shoes that can cause problems. Flip-flops, worn-out sneakers, and shoes that are too tight can all cause foot issues. To prevent future problems from her shoe choices, Sophia is following guidelines recommended by medical experts. The guidelines include:
Wearing shoes that fit well, have plenty of room in the toes, are supportive, and are comfortable right away. There should be no “break-in” period needed for shoes.
Avoiding high heels, especially those with heels over two inches high, or those that have narrow, pointed toe boxes or very thin heels.
If high heels must be worn, it should only be for a limited period of time.
As you have learned in this chapter, your skeletal system carries out a variety of important functions in your body, including physical support. But even though it is strong, your skeletal system can become damaged and deformed — even through such a seemingly innocuous act as wearing a certain type of shoe. Taking good care of your skeletal system is necessary to help it continue to take good care of the rest of you.
Attributions
This chapter is composed of text taken from of the following sources: