Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
9 Senses
9.1 Introduction
In this chapter you will learn about the human senses. Specifically, you will learn about:
How sensory mechanisms provide information about the external environment.
The different types of receptors and how they convert a stimulus into an action potential.
The location of receptors throughout the human body.
How receptors adapt to stimuli.
How visual information, sounds, smells, tastes, touch, and balance are detected by sensory receptor cells and then sent to the brain for interpretation.
9.2 Special and General Senses
The human body has two basic types of senses, called special senses and general senses. Special senses have specialized sense organs that gather sensory information and change it into nerve impulses. Special senses include vision (for which the eyes are the specialized sense organs), hearing (ears), balance (ears), taste (tongue), and smell (nasal passages). Somatic (General) senses, in contrast, are all associated with the sense of touch. They lack special sense organs. Instead, sensory information about touch is gathered by the skin and other body tissues, all of which have important functions besides gathering sense information. Whether the senses are special or general, however, they all depend on cells called sensory receptors.
SENSORY RECEPTORS
A sensory receptor is a specialized nerve cell that responds to a stimulus in the internal or external environment by generating a nerve impulse. The nerve impulse then travels along the sensory (afferent) nerve to the central nervous system for processing and to form a response.
There are several different types of sensory receptors that respond to different kinds of stimuli:
Mechanoreceptors respond to mechanical forces, such as pressure, roughness, vibration, and stretching. Most mechanoreceptors are found in the skin and are needed for the sense of touch. Mechanoreceptors are also found in the inner ear, where they are needed for the senses of hearing and balance.
Thermoreceptors respond to variations in temperature. They are found mostly in the skin and detect temperatures that are above or below body temperature.
Pain receptors (also called Nociceptors) respond to potentially damaging stimuli, which are generally perceived as pain. They are found in internal organs, as well as on the surface of the body. Different nociceptors are activated depending on the particular stimulus. Some detect damaging heat or cold, others detect excessive pressure, and still others detect painful chemicals (such as very hot spices in food).
Photoreceptors detect and respond to light. Most photoreceptors are found in the eyes and are needed for the sense of vision.
Chemoreceptors respond to certain chemicals. They are found mainly in taste buds on the tongue — where they are needed for the sense of taste — and in nasal passages, where they are needed for the sense of smell.
9.3 Somatic (General) Senses
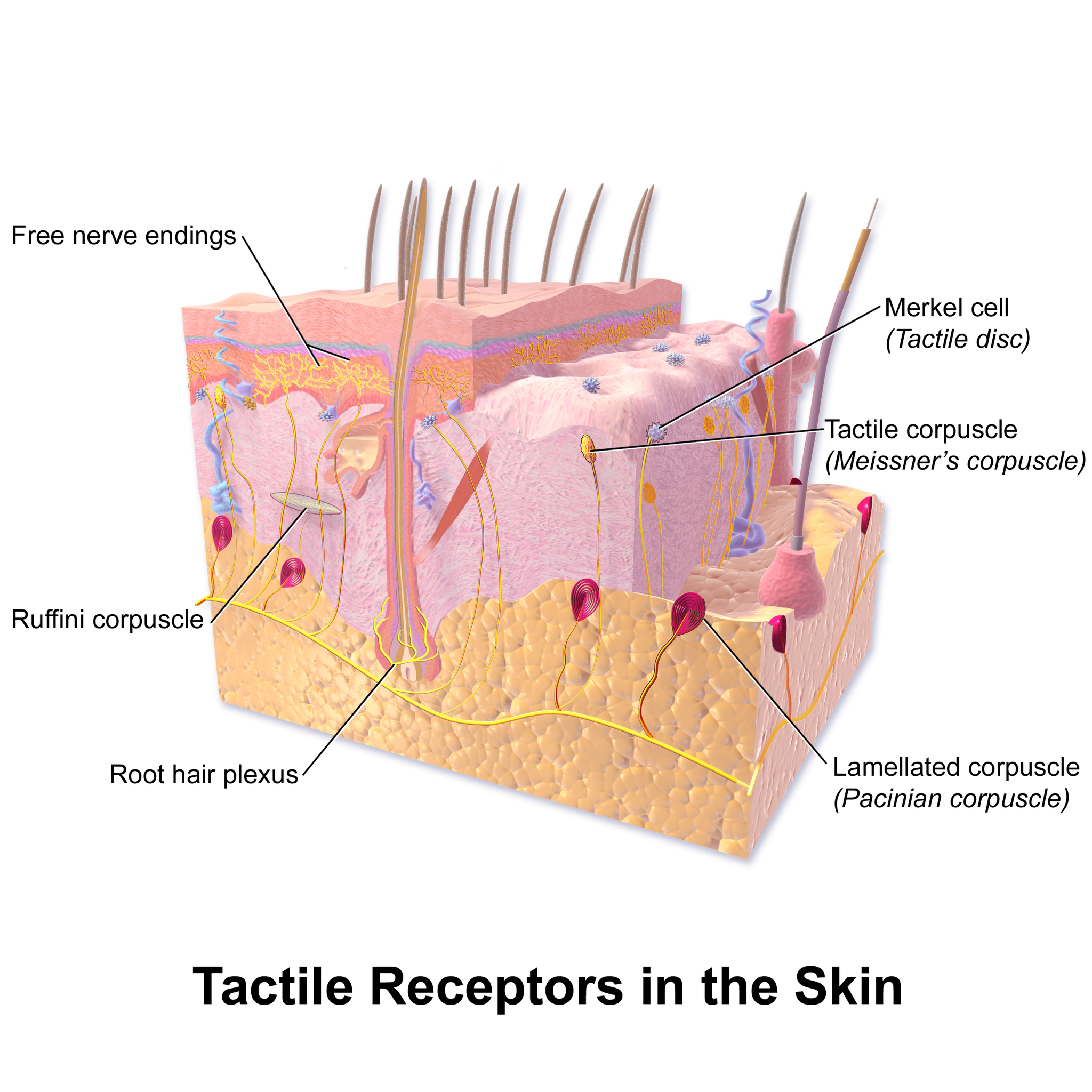
Somatic senses include sensations all over the body received from the skin, muscles, limbs and joints. It is also known as tactile sense, or more familiarly, as the sense of touch. Touch is the ability to sense pressure, vibration, temperature, pain, and other tactile stimuli. These types of stimuli are detected by mechanoreceptors, thermoreceptors, and nociceptors. Various types of tactile receptors in the skin are shown in Figure 9.1.
Figure 9.1 Tactile receptors in the skin include free nerve endings, Merkel cells, Meissner’s corpuscles, Pacinian corpuscles, root hair plexuses, and Ruffini corpuscles. Each type of sensory receptor responds to a different kind of tactile stimulus. For example, free nerve endings generally respond to pain and temperature variations, whereas Merkel cells are associated with the sense of light touch and the discrimination of shapes and textures.
Mechanoreceptors
Mechanoreceptors in the skin are described as encapsulated (that is, surrounded by a capsule) or unencapsulated (a group that includes free nerve endings). A free nerve ending, as its name implies, is an unencapsulated dendrite of a sensory neuron. Free nerve endings are the most common nerve endings in skin, and they extend into the middle of the epidermis. Free nerve endings are sensitive to painful stimuli, to hot and cold, and to light touch. They are slow to adjust to a stimulus and so are less sensitive to abrupt changes in stimulation.
There are four primary tactile mechanoreceptors in human skin: Merkel’s disks, Meissner’s corpuscles, Ruffini endings, and Pacinian corpuscle; two are located toward the surface of the skin and two are located deeper.
Merkel’s disks (shown in Figure 9.2) are found in the upper layers of skin near the base of the epidermis, both in skin that has hair and on hairless skin found on the palms and fingers, the soles of the feet, and the lips of humans and other primates. Merkel’s disks are densely distributed in the fingertips and lips. They are slow-adapting, encapsulated nerve endings, and they respond to light touch. Light touch, also known as discriminative touch, is a light pressure that allows the location of a stimulus to be pinpointed. The receptive fields of Merkel’s disks are small with well-defined borders. That makes them finely sensitive to edges and they come into use in tasks such as typing on a keyboard.
Figure 9.2 Four of the primary mechanoreceptors in human skin are shown. Merkel’s disks, which are unencapsulated, respond to light touch. Meissner’s corpuscles, Ruffini endings, Pacinian corpuscles are all encapsulated. Meissner’s corpuscles respond to touch and low-frequency vibration. Ruffini endings detect stretch, deformation within joints, and warmth. Pacinian corpuscles detect transient pressure and high-frequency vibration.
Meissner’s corpuscles, (shown in Figure 9.2) also known as tactile corpuscles, are found in the upper dermis, but they project into the epidermis. They, too, are found primarily in hairless skin on the fingertips and eyelids. They respond to fine touch and pressure, but they also respond to low-frequency vibration or flutter. They are rapidly adapting, fluid-filled, encapsulated neurons with small, well-defined borders and are responsive to fine details. Like Merkel’s disks, Meissner’s corpuscles are not as plentiful in the palms as they are in the fingertips.
Figure 9.3 Meissner corpuscles in the fingertips, such as the one viewed here using bright field light microscopy, allow for touch discrimination of fine detail. (credit: modification of work by “Wbensmith”/Wikimedia Commons; scale-bar data from Matt Russell).
Deeper in the epidermis, near the base, are Ruffini endings, which are also known as bulbous corpuscles. They are found in both hairless and hairy skin. These are slow-adapting, encapsulated mechanoreceptors that detect skin stretch and deformations within joints, so they provide valuable feedback for gripping objects and controlling finger position and movement. Thus, they also contribute to proprioception and kinesthesia. Ruffini endings also detect warmth. Note that these warmth detectors are situated deeper in the skin than are the cold detectors. It is not surprising, then, that humans detect cold stimuli before they detect warm stimuli.
Pacinian corpuscles (seen in Figure 9.4) are located deep in the dermis of both glabrous and hairy skin and are structurally similar to Meissner’s corpuscles; they are found in the bone periosteum, joint capsules, pancreas and other viscera, breast, and genitals. They are rapidly adapting mechanoreceptors that sense deep transient (but not prolonged) pressure and high-frequency vibration. Pacinian receptors detect pressure and vibration by being compressed, stimulating their internal dendrites. There are fewer Pacinian corpuscles and Ruffini endings in skin than there are Merkel’s disks and Meissner’s corpuscles.
Figure 9.4 Pacinian corpuscles, such as these visualized using bright field light microscopy, detect pressure (touch) and high-frequency vibration. (credit: modification of work by Ed Uthman; scale-bar data from Matt Russell).
Muscle spindles are stretch receptors that detect the amount of stretch or lengthening of muscles. Proprioceptive and kinesthetic signals come from limbs. Unconscious proprioceptive signals run from the spinal cord to the cerebellum, the brain region that coordinates muscle contraction, rather than to the thalamus, like most other sensory information.
In addition, there are also rapidly adapting hair receptors, which are found on nerve endings that wrap around the base of hair follicles. There are a few types of hair receptors that detect slow and rapid hair movement, and they differ in their sensitivity to movement. Some hair receptors also detect skin deflection, and certain rapidly adapting hair receptors allow detection of stimuli that have not yet touched the skin.
Integration of Signals from Mechanoreceptors
The configuration of the different types of receptors working in concert in human skin results in a very refined sense of touch. The nociceptive receptors—those that detect pain—are located near the surface. Small, finely calibrated mechanoreceptors—Merkel’s disks and Meissner’s corpuscles—are located in the upper layers and can precisely localize even gentle touch. The large mechanoreceptors—Pacinian corpuscles and Ruffini endings—are located in the lower layers and respond to deeper touch. (Consider that the deep pressure that reaches those deeper receptors would not need to be finely localized.) Both the upper and lower layers of the skin hold rapidly and slowly adapting receptors. Both primary somatosensory cortex and secondary cortical areas are responsible for processing the complex picture of stimuli transmitted from the interplay of mechanoreceptors.
Density of Mechanoreceptors
The distribution of touch receptors in human skin is not consistent over the body. In humans, touch receptors are less dense in skin covered with any type of hair, such as the arms, legs, torso, and face. Touch receptors are denser in hairless skin (the type found on human fingertips and lips, for example), which is typically more sensitive and is thicker than hairy skin (4 to 5 mm versus 2 to 3 mm).
How is receptor density estimated in a human subject? The relative density of pressure receptors in different locations on the body can be demonstrated experimentally using a two-point discrimination test. In this demonstration, two sharp points, such as two thumbtacks, are brought into contact with the subject’s skin (though not hard enough to cause pain or break the skin). The subject reports if he or she feels one point or two points. If the two points are felt as one point, it can be inferred that the two points are both in the receptive field of a single sensory receptor. If two points are felt as two separate points, each is in the receptive field of two separate sensory receptors. The points could then be moved closer and re-tested until the subject reports feeling only one point, and the size of the receptive field of a single receptor could be estimated from that distance.
Thermoreceptors
There are different types of cold receptors on some free nerve endings: thermoreceptors, located in the dermis, skeletal muscles, liver, and hypothalamus, that are activated by different temperatures. Their pathways into the brain run from the spinal cord through the thalamus to the primary somatosensory cortex. Warmth and cold information from the face travels through one of the cranial nerves to the brain. You know from experience that a tolerably cold or hot stimulus can quickly progress to a much more intense stimulus that is no longer tolerable. Any stimulus that is too intense can be perceived as pain because temperature sensations are conducted along the same pathways that carry pain sensations
The thermoreceptors located in the dermis of the skin provide information about the external environment and adapt quickly. Thermoreceptors in the abdominal and thoracic regions of the body monitor the internal temperature of the body and adapt slowly to maintain homeostasis.
Pain
Pain is the name given to nociception, which is the neural processing of injurious stimuli in response to tissue damage. Pain is caused by true sources of injury, such as contact with a heat source that causes a thermal burn or contact with a corrosive chemical. But pain also can be caused by harmless stimuli that mimic the action of damaging stimuli, such as contact with capsaicins, the compounds that cause peppers to taste hot and which are used in self-defense pepper sprays and certain topical medications. Peppers taste “hot” because the protein receptors that bind capsaicin open the same calcium channels that are activated by warm receptors.
Nociception starts at the sensory receptors, but pain, inasmuch as it is the perception of nociception, does not start until it is communicated to the brain. There are several nociceptive pathways to and through the brain. Most axons carrying nociceptive information into the brain from the spinal cord project to the thalamus (as do other sensory neurons) and the neural signal undergoes final processing in the primary somatosensory cortex. Interestingly, one nociceptive pathway projects not to the thalamus but directly to the hypothalamus in the forebrain, which modulates the cardiovascular and neuroendocrine functions of the autonomic nervous system. Threatening—or painful—stimuli stimulate the sympathetic branch of the visceral sensory system, readying a fight-or-flight response.
Review
Compare and contrast special senses and general senses.
What are sensory receptors?
Identify a mechanoreceptor used in two different human senses. Describe the type of mechanical stimuli that each detects.
If you were to burn your epidermis, what receptor type would you most likely burn?
free nerve endings
Ruffini endings
Pacinian corpuscle
hair receptors
What is the difference between a free nerve ending and an encapsulated nerve ending?
What are the four primary tactile mechanoreceptors in human skin? Be able to distinguish between them.
Where are thermoreceptors found?
What is pain and why is it necessary?
List five types of sensory receptors and the type of stimulus each detects.
9.4 Special Senses
Taste and Smell
Taste (also called gustation) and smell (olfaction) are both abilities to sense chemicals, so taste and olfactory (odor) receptors are chemoreceptors. Both types of chemoreceptors send nerve impulses to the brain along sensory nerves, and the brain “tells” us what we are tasting or smelling. They are the most interconnected senses in that both involve molecules of the stimulus entering the body and bonding to receptors. Smell lets an animal sense the presence of food other chemicals in the environment that can impact their survival. Similarly, the sense of taste allows animals to discriminate between types of foods. While the value of a sense of smell is obvious, what is the value of a sense of taste? Different tasting foods have different attributes, both helpful and harmful. For example, sweet-tasting substances tend to be highly caloric, which could be necessary for survival in lean times. Bitterness is associated with toxicity, and sourness is associated with spoiled food. Salty foods are valuable in maintaining homeostasis by helping the body retain water and by providing ions necessary for cells to function.
Both tasting abilities and sense of smell change with age. In humans, the senses decline dramatically by age 50 and continue to decline. A child may find a food to be too spicy, whereas an elderly person may find the same food to be bland and unappetizing.
TASTE
Detecting a taste (gustation) is relies on chemical receptors being stimulated by certain molecules. The primary organ of taste is the taste bud. A taste bud is a cluster of gustatory receptors (taste cells) that are located within the bumps on the tongue called papillae (singular: papilla).
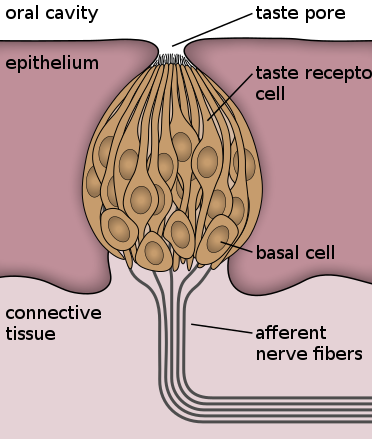
Each taste bud’s taste cells are replaced every 10 to 14 days. These are elongated cells with hair-like processes called microvilli at the tips that extend into the taste bud pore. Food molecules (tastants) are dissolved in saliva, and they bind with and stimulate the receptors on the microvilli. The receptors for tastants are located across the outer portion and front of the tongue. You can see a diagram of a taste receptor cell and related structures in Figure 9.5. Taste receptor cells make contact with chemicals in food through tiny openings called taste pores. When certain chemicals bind with taste receptor cells, it generates nerve impulses that travel through afferent nerves to the CNS.
In humans, there are five primary tastes, and each taste has only one corresponding type of receptor. Thus, each receptor is specific to its stimulus (tastant). There are taste receptors for sweet, salty, sour, bitter, and meaty tastes. The meaty or savory taste is called umami.
The identification of umami as a fundamental taste occurred fairly recently— it was identified in 1908 by Japanese scientist Kikunae Ikeda while he worked with seaweed broth, but it was not widely accepted as a taste that could be physiologically distinguished until many years later. The taste of umami, also known as savoriness, is attributable to the taste of the amino acid L-glutamate. In fact, monosodium glutamate, or MSG, is often used in cooking to enhance the savory taste of certain foods. What is the adaptive value of being able to distinguish umami? Savory substances tend to be high in protein.
Figure 9.5 Taste receptor cells are in taste buds on the tongue. Taste pore exposes these cells into the oral cavity. Basal cells are not involved in tasting but differentiate into taste receptor cells.
SMELL
All odors that we perceive are molecules in the air we breathe. If a substance does not release molecules into the air from its surface, it has no smell. And if a human or other animal does not have a receptor that recognizes a specific molecule, then that molecule has no smell. Humans have millions of olfactory receptors that work in various combinations to allow us to sense about 10,000 different odors. Compare that to mice, for example, which have about 1,300 olfactory receptor types, and therefore probably sense more odors. Both odors and tastes involve molecules that stimulate specific chemoreceptors. Although humans commonly distinguish taste as one sense and smell as another, they work together to create the perception of flavor. A person’s perception of flavor is reduced if he or she has congested nasal passages. Did you ever notice that food seems to have less taste when you have a stuffy nose? This occurs because the sense of smell contributes to the sense of taste, and a stuffy nose interferes with the ability to smell.
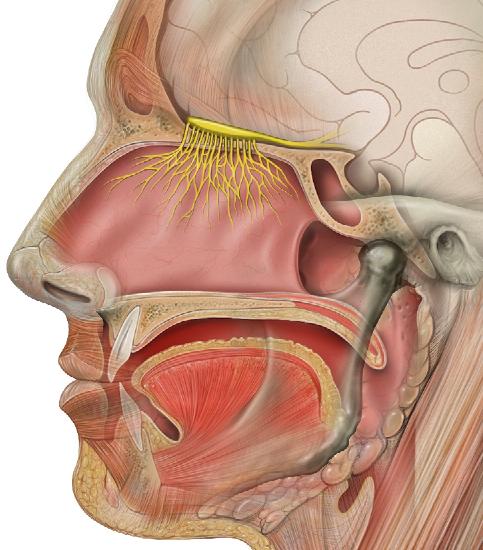
Olfactory receptors line the passages inside the nasal passages (Figure 9.6). Odorants (odor molecules) enter the nose and dissolve in the olfactory epithelium, the mucosa at the back of the nasal cavity. The olfactory epithelium is a collection of specialized olfactory receptors in the back of the nasal cavity. Recall that sensory cells are neurons. An olfactory receptor, which is a dendrite of a specialized neuron, responds when it binds certain molecules inhaled from the environment by sending impulses directly to the olfactory bulb of the brain.
Olfactory neurons are bipolar neurons (neurons with two processes from the cell body). Each neuron has a single dendrite buried in the olfactory epithelium, and extending from this dendrite are 5 to 20 receptor-laden, hair-like cilia that trap odorant molecules. The sensory receptors on the cilia are proteins, and it is the variations in their amino acid chains that make the receptors sensitive to different odorants. Each olfactory sensory neuron has only one type of receptor on its cilia, and the receptors are specialized to detect specific odorants, so the bipolar neurons themselves are specialized. When an odorant binds with a receptor that recognizes it, the sensory neuron associated with the receptor is stimulated. Olfactory stimulation is the only sensory information that directly reaches the cerebral cortex, whereas other sensations are relayed through the thalamus.
Figure 9.6: The yellow structures inside this drawing of the nasal passages are an olfactory nerve with many nerve endings. The nerve endings are located at the roof of the nasal cavity. The nerve endings sense chemicals in the air as it passes through the nasal cavities.Watch this following video for more information on Taste and Smell.
Taste and smell are interconnected senses. True or False.
_____________ is the primary organ of taste.
What are the primary tastes and where are they located?
What is umami?
_______________ is the portion of the brain that receives the signals for the sense of smell.
There are more taste receptors than smell receptors. True or False.
What receptors line the nasal passages?
HEARING
Hearing is the ability to sense sound waves, and the ear is the organ that senses sound.
Hearing is important to humans and to other animals for many different interactions. It enables an organism to detect and receive information about danger, such as an approaching predator, and to participate in communal exchanges like those concerning territories or mating. On the other hand, although it is physically linked to the auditory system, the vestibular system is not involved in hearing. Instead, an animal’s vestibular system detects its own movement, both linear and angular acceleration and deceleration, and balance.
Sound
Auditory stimuli are sound waves, which are mechanical, pressure waves that move through a medium, such as air or water. There are no sound waves in a vacuum since there are no air molecules to move in waves. The speed of sound waves differs, based on altitude, temperature, and medium, but at sea level and a temperature of 20° C (68° F), sound waves travel in the air at about 343 meters per second.
As is true for all waves, there are four main characteristics of a sound wave: frequency, wavelength, period, and amplitude. Frequency is the number of waves per unit of time, and in sound is heard as pitch. High-frequency (=15.000Hz) sounds are higher-pitched (short wavelength) than low frequency (long wavelengths; <100Hz) sounds. Frequency is measured in cycles per second, and for sound, the most commonly used unit is hertz (Hz), or cycles per second. Most humans can perceive sounds with frequencies between 30 and 20,000 Hz. Women are typically better at hearing high frequencies, but everyone’s ability to hear high frequencies decreases with age. Dogs detect up to about 40,000 Hz; cats, 60,000 Hz; bats, 100,000 Hz; and dolphins 150,000 Hz, and American shad, a fish, can hear 180,000 Hz. Those frequencies above the human range are called ultrasound.
Amplitude, or the dimension of a wave from peak to trough, in sound is heard as volume and is illustrated in [link]. The sound waves of louder sounds have greater amplitude than those of softer sounds. For sound, volume is measured in decibels (dB). The softest sound that a human can hear is the zero point. Humans speak normally at 60 decibels.
Figure 9.7: For sound waves, wavelength corresponds to pitch. Amplitude of the wave corresponds to volume.
Reception of Sound
Sound waves are collected by the external, cartilaginous part of the ear called the pinna, then travel through the auditory canal and cause vibration of the thin diaphragm called the tympanic membrane or ear drum, the innermost part of the outer ear (Figure 9.8). Interior to the tympanum is the middle ear. The middle ear holds three small bones called the ossicles, which transfer energy from the moving tympanum to the inner ear. The three ossicles are the malleus (also known as the hammer), the incus (the anvil), and stapes (the stirrup). The three ossicles are unique to mammals, and each plays a role in hearing. The malleus attaches at three points to the interior surface of the tympanic membrane. These bones also function to collect force and amplify sounds.
From the middle ear, the vibrations pass to the cochlea in the inner ear. The cochlea is a coiled tube filled with liquid. The liquid moves in response to the vibrations, causing tiny hair cells (which are mechanoreceptors) lining the cochlea to bend. In response, the hair cells send nerve impulses to the auditory nerve, which carries the impulses to the brain. The brain interprets the impulses and “tells” us what we are hearing.
Figure 9.8 Most of the structures of the ear are involved in hearing. Only the semicircular canals are not involved in hearing. Instead, they sense head position, which is used to monitor balance.
Transduction of Sound
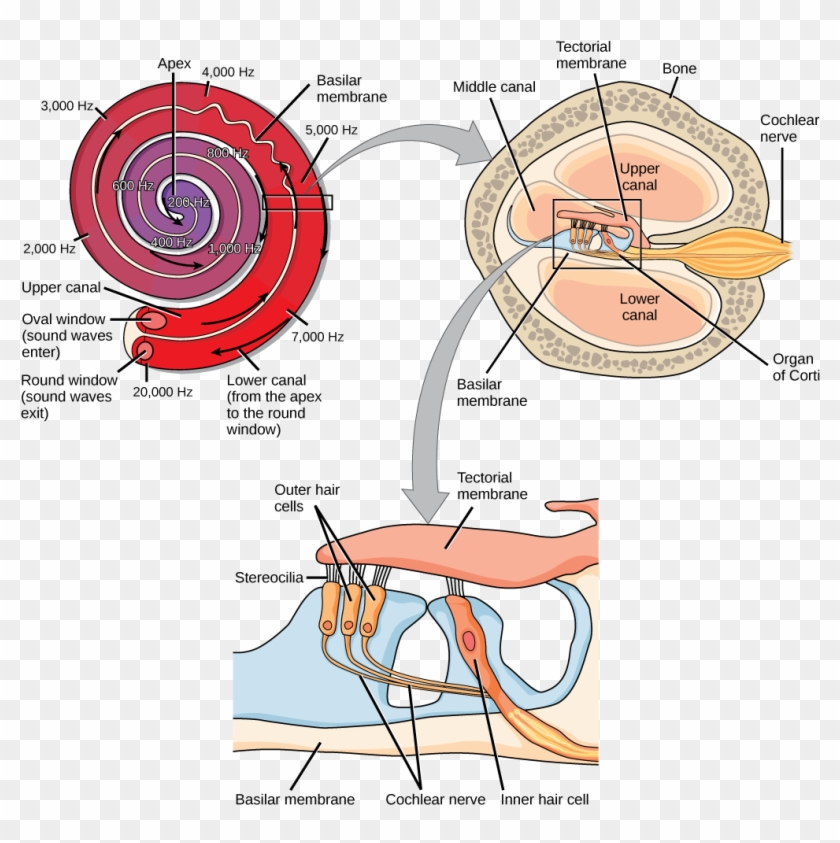
Vibrating objects, such as vocal cords, create sound waves or pressure waves in the air. When these pressure waves reach the ear, the ear transduces this mechanical stimulus (pressure wave) into a nerve impulse (electrical signal) that the brain perceives as sound. The pressure waves strike the tympanum, causing it to vibrate. The mechanical energy from the moving tympanum transmits the vibrations to the three bones of the middle ear. The stapes transmits the vibrations to a thin diaphragm called the oval window, which is the outermost structure of the inner ear. The structures of the inner ear are found in the cochlea, a bony, hollow structure that is the most interior portion of the ear. Here, the energy from the sound wave is transferred from the stapes through the flexible oval window and to the fluid of the cochlea. The vibrations of the oval window create pressure waves in the fluid inside the cochlea. The cochlea is a whorled structure, like the shell of a snail, and it contains receptors for transduction of the mechanical wave into an electrical signal (as illustrated in [link]). Inside the cochlea, the basilar membrane is a mechanical analyzer that runs the length of the cochlea, curling toward the cochlea’s center.
The mechanical properties of the basilar membrane change along its length, such that it is thicker, tauter, and narrower at the outside of the whorl (where the cochlea is largest), and thinner, floppier, and broader toward the apex, or center, of the whorl (where the cochlea is smallest). Different regions of the basilar membrane vibrate according to the frequency of the sound wave conducted through the fluid in the cochlea. For these reasons, the fluid-filled cochlea detects different wave frequencies (pitches) at different regions of the membrane. When the sound waves in the cochlear fluid contact the basilar membrane, it flexes back and forth in a wave-like fashion. Above the basilar membrane is the tectorial membrane.
The site of transduction is in the organ of Corti. It is composed of hair cells held in place above the basilar membrane like flowers projecting up from soil, with their exposed short, hair-like stereocilia contacting or embedded in the tectorial membrane above them. The inner hair cells are the primary auditory receptors and exist in a single row, numbering approximately 3,500. All of the stereocilia are mechanoreceptors, and when bent by vibrations they respond by opening a gated ion channel. As a result, the hair cell membrane is depolarized, and a signal is transmitted to the cochlear nerve. Intensity (volume) of sound is determined by how many hair cells at a particular location are stimulated.
When sound waves produce fluid waves inside the cochlea, the basilar membrane flexes, bending the stereocilia that attach to the tectorial membrane. Their bending results in action potentials in the hair cells, and auditory information travels along auditory nerve to the brain.
Figure 9.9 In the human ear, sound waves cause the stapes to press against the oval window. Vibrations travel up the fluid-filled interior of the cochlea. The basilar membrane that lines the cochlea gets continuously thinner toward the apex of the cochlea. Different thicknesses of membrane vibrate in response to different frequencies of sound. Sound waves then exit through the round window. In the cross section of the cochlea (top right figure), note that in addition to the upper canal and lower canal, the cochlea also has a middle canal. The organ of Corti (bottom image) is the site of sound transduction. Movement of stereocilia on hair cells results in an action potential that travels along the auditory nerve.
The Science of Hearing.
Vestibular Apparatus
The stimuli associated with the vestibular apparatus are gravity, balance, position of head, acceleration and deceleration. Gravity, acceleration, and deceleration are detected by evaluating the inertia on receptive cells in the vestibular system. Gravity is detected through head position. Acceleration and deceleration are expressed through turning or tilting of the head.
The vestibular system has some similarities with the auditory system. It utilizes hair cells just like the auditory system, but it excites them in different ways. There are five vestibular receptor organs in the inner ear: the utricle, the saccule, and three semicircular canals. Together, they make up what’s known as the vestibular apparatus. The utricle and saccule respond to acceleration in a straight line, such as gravity. The roughly 30,000 hair cells in the utricle and 16,000 hair cells in the saccule lie below a gelatinous layer, with their stereocilia projecting into the gelatin. Embedded in this gelatin are calcium carbonate crystals—like tiny rocks. When the head is tilted, the crystals continue to be pulled straight down by gravity, but the new angle of the head causes the gelatin to shift, thereby bending the stereocilia. The bending of the stereocilia stimulates the neurons, and they signal to the brain that the head is tilted, allowing the maintenance of balance. It is the vestibular branch of the vestibulocochlear cranial nerve that deals with balance. Balance is the ability to sense and maintain an appropriate body position.
The fluid-filled semicircular canals are tubular loops set at oblique angles. They are arranged in three spatial planes. The base of each canal has a swelling that contains a cluster of hair cells. The hairs project into a gelatinous cap called the cupula and monitor angular acceleration and deceleration from rotation. They would be stimulated by driving your car around a corner, turning your head, or falling forward. One canal lies horizontally, while the other two lie at about 45-degree angles to the horizontal axis. When the brain processes input from all three canals together, it can detect angular acceleration or deceleration in three dimensions. When the head turns, the fluid in the canals shifts, thereby bending stereocilia and sending signals to the brain. Upon cessation accelerating or decelerating—or just moving—the movement of the fluid within the canals slows or stops. For example, imagine holding a glass of water. When moving forward, water may splash backwards onto the hand, and when motion has stopped, water may splash forward onto the fingers. While in motion, the water settles in the glass and does not splash. Note that the canals are not sensitive to velocity itself, but to changes in velocity, so moving forward at 60mph with your eyes closed would not give the sensation of movement, but suddenly accelerating or braking would stimulate the receptors.
Review
What is the difference between frequency and amplitude of a sound wave?
The ___________, _______________, and ______________ are the parts of the outer ear.
What are the three bones of the inner ear?
Describe the pathway of sound waves from the pinna to the oval window.
What is the cochlea and how does it change mechanical energy into an action potential?
Which of the following are found both in the auditory system and the vestibular system?
basilar membrane
hair cells
semicircular canals
ossicles
What is the function of the semicircular canals?
Explain how structures of the ear collect and amplify sound waves and transform them to nerve impulses.
What role does the ear play in balance? Which structures of the ear are involved in balance?
What Is Vertigo & Why Do We Get It?
Vision
Vision (or sight) is the ability to sense light and see. The eye is the special sensory organ that collects and focuses light and forms images. The eye, however, is not sufficient for us to see. The brain also plays a necessary role in vision. Vision is our primary sense and more than 50 per cent of the cerebral cortex is devoted to processing visual information. A person with normal color vision can differentiate between hundreds of thousands of different colors, hues, and shades.
Figure 9.10 The human eye is a sensory organ that collects and focusses light, forms images, and changes them to nerve impulses.
HOW THE EYE WORKS
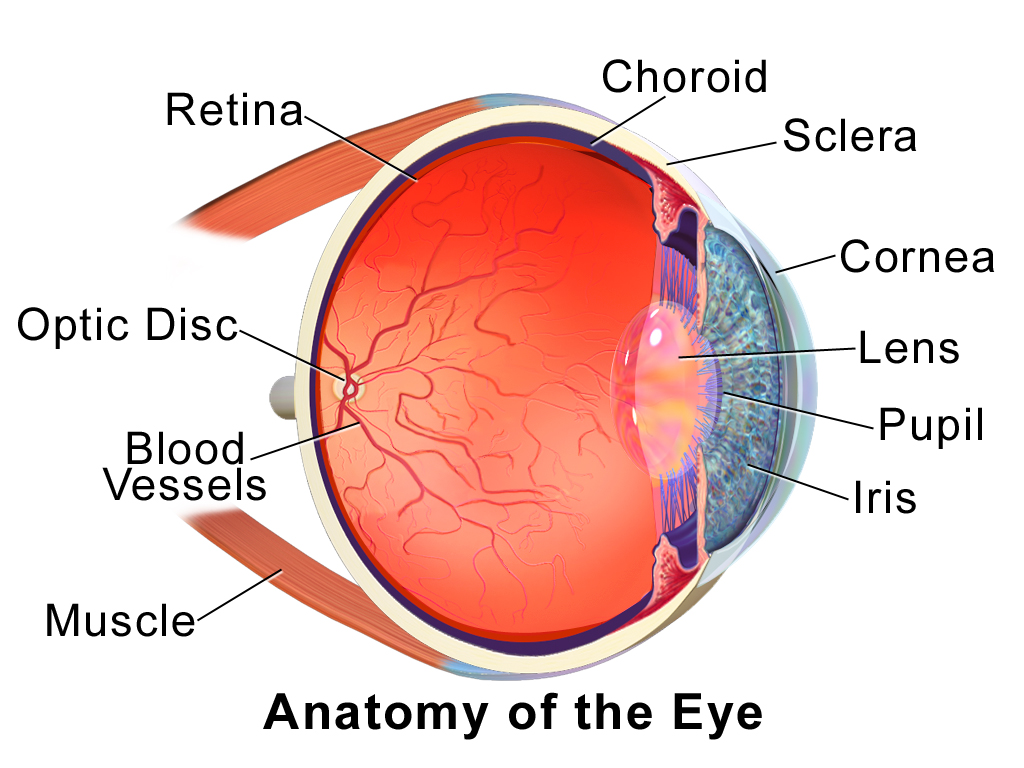
Figure 9.11 (below) shows the anatomy of the human eye in cross-section. The eye gathers and focuses light to form an image, and then changes the image to nerve impulses that travel to the brain. The eye’s functions are summarized in the following steps.
Light passes first through the cornea, which is a clear convex outer layer that protects the eye and helps to focus the light by refracting (or bending) it.
Next, light enters the interior of the eye through an opening called the pupil. The size of this opening is controlled by the colored part of the eye (called the iris), which adjusts the size based on the brightness of the light. The iris causes the pupil to narrow in bright light and widen in dim light. Filling the space between the cornea and the iris is a semi-gelatinous fluid called aqueoushumor and functions to maintain the shape of the eye. In conditions of high ambient light, the iris contracts, reducing the size of the pupil at its center. In conditions of low light, the iris relaxes, and the pupil enlarges.
The light then passes through the lens, which refracts the light even more and focuses it on the retina at the back of the eye, as an inverted image. Sitting behind the lens is a gelatinous fluid called vitreous humor, which functions to maintain the shape of the eye.
The retina (the inner layer of the eye) contains two types of photoreceptors: rod and cone cells. Rod cells, which are found mainly in all areas of the retina other than the very center, are particularly sensitive to low levels of light. Cone cells, which are found mainly in the center of the retina, are sensitive to light of different colors, and allow color vision. The rods and cones convert the light that strikes them to nerve impulses.
The nerve impulses from the rods and cones travel to the optic nerve via the optic disc (also known as the optic nerve), which is a circular area at the back of the eye where the optic nerve connects to the retina.
Figure 9.11 Trace the path of light through the eye as you read about in the five steps above.
Photoreceptor cells
The photoreceptive cells of the eye, where transduction of light to nervous impulses occurs, are located in the retina (shown in figure 9.11) on the inner surface of the back of the eye. But light does not impinge on the retina unaltered. It passes through other layers that process it so that it can be interpreted by the retina. Visual signals leave the cones and rods, travel to the bipolar cells, and then to ganglion cells. A large degree of processing of visual information occurs in the retina itself, before visual information is sent to the brain.
Layers of the retina:
Outermost layer contains pigmented cells that absorb excess light.
Photoreceptor cells (rods and cones)
Bipolar cells – synapse with the photoreceptor cells and partially process information.
Ganglion cells make up the innermost layer. the axons of these cells make up the optic nerve.
Figure 9.12 (a) The human eye is shown in cross section. (b) A blowup shows the layers of the retina.
There are two types of photoreceptors in the retina: rods and cones, named for their general appearance as illustrated in Figure 9.13. Both rods and cones contain photopigments.
Rods detect shades of gray, are strongly photosensitive and are located in the outer edges of the retina. They detect dim light and are used primarily for peripheral and nighttime vision. Rods contain the photopigment rhodopsin. Rhodopsin, has two main parts. When light hits a photoreceptor, it causes a shape change in one of the parts, altering its structure. In bright light the rhodopsin breaks down and the rods stop functioning.
Cones are weakly photosensitive and are located near the center of the retina. They respond to bright light, and their primary role is in daytime, color vision. Humans have color vision because we have three types of cone cells: blue, green and red. Each of these types of cone cell detects a specific wavelength of light, for which they are named. The combined stimulus is then perceived as a specific color, based on the ratio of the amount stimulus coming from each of the three types of cone cells.
Figure 9.13 Rods and cones are photoreceptors in the retina. Rods respond in low light and can detect only shades of gray. Cones respond in intense light and are responsible for color vision.
In the absence of light, the bipolar neurons that connect rods and cones to ganglion cells are continuously and actively inhibited by the rods and cones. Exposure of the retina to light hyperpolarizes the rods and cones and removes their inhibition of bipolar cells. The now active bipolar cells in turn stimulate the ganglion cells, which send action potentials along their axons (which leave the eye as the optic nerve). Thus, the visual system relies on change in retinal activity, rather than the absence or presence of activity, to encode visual signals for the brain.
ROLE OF THE BRAIN IN VISION
The optic nerves from both eyes meet and cross just below the bottom of the hypothalamus in the brain. The information from both eyes is sent to the visual cortex in the occipital lobe of the cerebrum, which is part of the cerebral cortex. The visual cortex is the largest system in the human brain and is responsible for processing visual images. It interprets messages from both eyes and “tells” us what we are seeing.
REGULATING LIGHT AND FOCUS
The main function of the lens is to focus light on the retina and fovea centralis. The lens is dynamic, focusing and re-focusing light as the eye rests on near and far objects in the visual field. The lens is operated by muscles that stretch it flat or allow it to thicken, changing the focal length of light coming through it to focus it sharply on the retina. With age comes the loss of the flexibility of the lens, and a form of farsightedness called presbyopia results.
The fovea is the region in the center back of the eye that is responsible for acute vision. The fovea has a high density of cones. When you bring your gaze to an object to examine it intently in bright light, the eyes orient so that the object’s image falls on the fovea. However, when looking at a star in the night sky or other object in dim light, the object can be better viewed by the peripheral vision because it is the rods at the edges of the retina, rather than the cones at the center, that operate better in low light. In humans, cones far outnumber rods in the fovea.
VISION PROBLEMS
Figure 9.14 The three vision problems described are typically solved by using glasses.
Vision problems are very common. Three of the most common are myopia,hyperopia, andastigmatism and they often start in childhood or adolescence. Another common problem, called presbyopia, occurs in most people, beginning in middle adulthood. In all three conditions, the eyes fail to focus images correctly on the retina, resulting in blurred vision.
Myopia
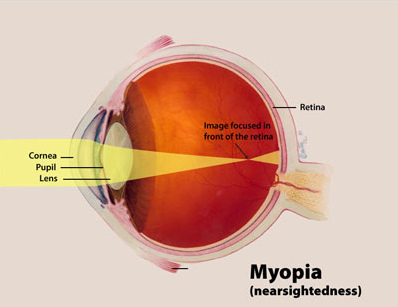
Figure 9.15 In a patient who is nearsighted, the image is focused in front of the retina, resulting in distant objects appearing out of focus.
Myopia (or nearsightedness) occurs when the light that comes into the eye does not directly focus on the retina, but in front of it, as shown in Figure 9.15. It occurs when an eyeball is elongated. As a result, distant objects may appear out of focus, but the focus of close objects is not affected. Myopia may occur because the eyeball is elongated from front to back, or because the cornea is too curved. Myopia can be corrected with the use of corrective lenses, either eyeglasses or contact lenses. Myopia can also be corrected by refractive surgery performed with a laser.
Hyperopia
Figure 9.16 In a patient who exhibits hyperopia, the image focuses at a point somewhere behind the retina, causing close objects to appear blurry.
Hyperopia (or farsightedness) happens when the light coming into the eye does not directly focus on the retina but behind it, as shown in Figure 9.16. It is caused by an eyeball that is too short. This causes close objects to appear out of focus but does not affect the focus of distant objects. Hyperopia may occur because the eyeball is too short from front to back, or because the lens is not curved enough. Hyperopia can be corrected through the use of corrective lenses or laser surgery.
Astigmatism
Astigmatism occurs when the lens and/or the cornea have an irregular shape. This results in a scattering of light onto the retina and the image is not focused evenly. this can be corrected with specialized lenses to accommodate for the irregularly shaped parts.
Presbyopia
Presbyopia is a vision problem associated with aging, in which the eye gradually loses its ability to focus on close objects. The precise origin of presbyopia is not known for certain, but evidence suggests that the lens may become less elastic with age, causing the muscles that control the lens to lose power as people grow older. The first signs of presbyopia — eyestrain, difficulty seeing in dim light, problems focusing on small objects and fine print — are usually first noticed between the ages of 40 and 50. Most older people with this problem use corrective lenses to focus on close objects, because surgical procedures to correct presbyopia have not been as successful as those for myopia and hyperopia.
Review
How is the relationship between photoreceptors and bipolar cells different from other sensory receptors and adjacent cells?2.
When you see colors, what receptor cells are activated? Where are these receptors located? What lobe of the brain is primarily used to process visual information?
Describe the pathway of light through the eye.
How is light regulated in the eye? What structures are involved?
What is the difference between myopia and hyperopia?
What happens when light hits the rods?
Why do people over 55 often need reading glasses?
Their cornea no longer focuses correctly.
Their lens no longer focuses correctly.
Their eyeball has elongated with age, causing images to focus in front of their retina.
Their retina has thinned with age, making vision more difficult.
Vision: Crash Course Anatomy & Physiology #18
Attributions
This chapter is composed of text taken from of the following sources:
CrashCourse. Taste & Smell: Crash Course Anatomy & Physiology #16. YouTube, uploaded by CrashCourse, Year, Month Day. Available at: https://www.youtube.com/watch?v=[video_id]
OER Commons. (2018, August 2). [Title of the resource]. [Subject: Applied Science, Life Science, Biology]. [Creative Commons Attribution Non-Commercial License]. Retrieved from https://www.oercommons.org/courseware/lesson/15125
Oliver, D. L. (2018). The science of hearing [Video]. TED-Ed. YouTube. Retrieved from https://youtu.be/LkGOGzpbrCk