Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
11 Heart and Blood Vessels
11.1 INTRODUCTION
In this chapter, you will learn about the cardiovascular system, which transports substances throughout the body. Specifically, you will learn about:
The major components of the cardiovascular system: the heart and blood vessels.
The functions of the cardiovascular system.
How blood is oxygenated through the pulmonary circulation, which transports blood between the heart and lungs.
How blood is circulated throughout the body through the systemic circulation.
Types of blood vessels — including arteries, veins, and capillaries — and their functions, similarities, and differences.
The structure of the heart, how it pumps blood, and how contractions of the heart are controlled.
What blood pressure is and how it is regulated.
Cardiovascular diseases (including heart attack, stroke, and angina), and the risk factors and precursors — such as high blood pressure and atherosclerosis — that contribute to them.
11.2 WHAT IS THE CARDIOVASCULAR SYSTEM?
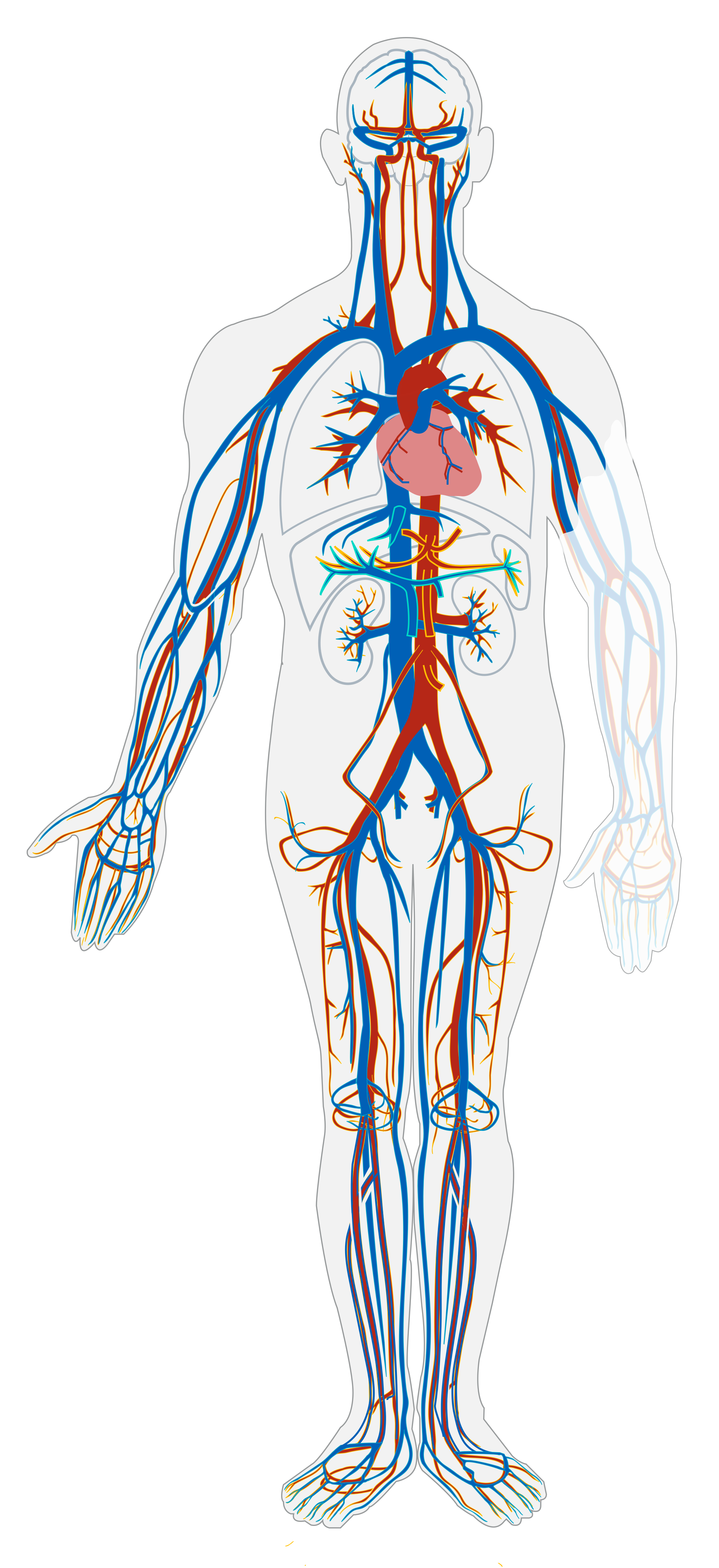
The cardiovascular system, also called the circulatory system, is the organ system that transports materials to and from all the cells of the body. The materials carried by the cardiovascular system include oxygen from the lungs, nutrients from the digestive system, hormones from glands of the endocrine system, and waste materials from cells throughout the body. Transport of these and many other materials is necessary to maintain homeostasis of the body. The main components of the cardiovascular system are the heart, blood vessels, and blood. Each of these components is shown in Figure 11.1 below.
Figure 11.1 This simplified drawing of the cardiovascular system shows its main structures. The heart is shown in the chest in red. Blood vessels called arteries are also shown in red, and blood vessels called veins are shown in blue.
The heartis a muscular organ in the chest. It consists mainly of cardiac muscle tissue, and it pumps blood through blood vessels by repeated, rhythmic contractions. The blood vessels of the cardiovascular system are like a network of interconnected, one-way roads that range from superhighways to back alleys. Like a network of roads, the blood vessels are tasked with allowing the transport of materials from one place to another.
11.3 TYPES OF BLOOD VESSELS
Blood vessels are the part of the cardiovascular system that transports blood throughout the human body. There are three major types of blood vessels. Besides veins, they include arteries and capillaries.
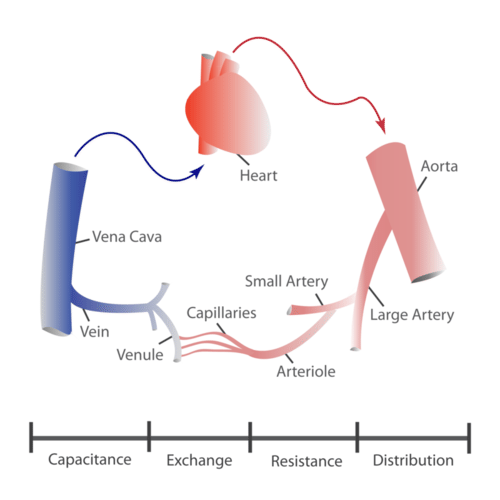
Figure 11.2 This diagram represents the structure and functions of the different types of blood vessels in the cardiovascular system.
ARTERIES
Arteriesare defined as blood vessels that carry blood away from the heart. Blood flows through arteries largely because it is under pressure from the pumping action of the heart. It should be noted that coronary arteries, which supply heart muscle cells with blood, travel toward the heart, but not as part of the blood flow that travels through the chambers of the heart. Most arteries, including coronary arteries, carry oxygenated blood, but there are a few exceptions, most notably the pulmonary artery. This artery carries deoxygenated blood from the heart to the lungs, where it picks up oxygen and releases carbon dioxide. In virtually all other arteries, the hemoglobin in red blood cells is highly saturated with oxygen (95–100 per cent). These arteries distribute oxygenated blood to tissues throughout the body.
The largest artery in the body is the aorta, which is connected to the heart and extends down into the abdomen (see Figure 11.2). The aorta has high-pressure, oxygenated blood pumped directly into it from the left ventricle of the heart. The aorta has many branches, and the branches subdivide repeatedly, with the subdivisions growing smaller and smaller in diameter. The smallest arteries are called arterioles.
VEINS
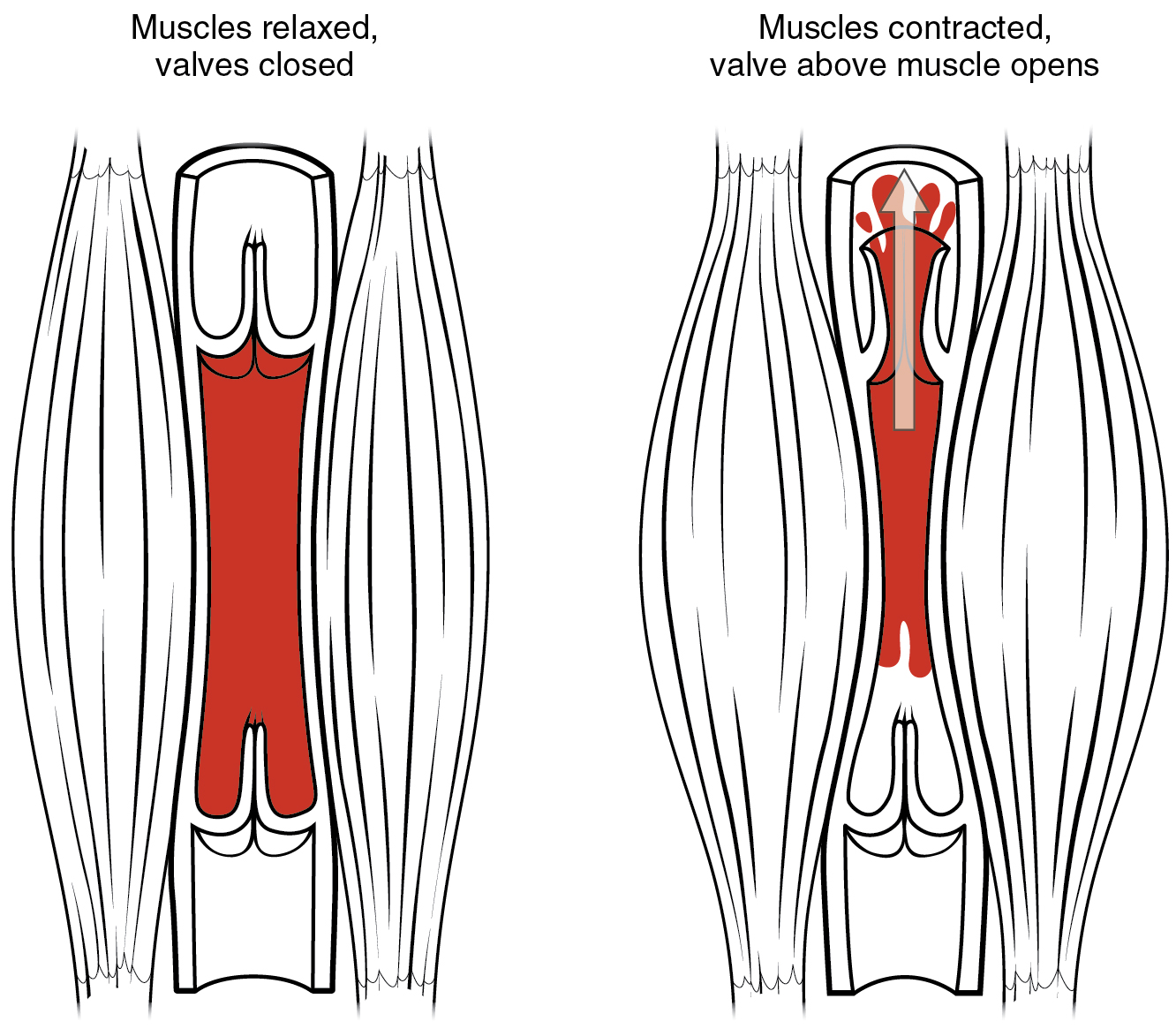
Veins are defined as blood vessels that carry blood toward the heart. Blood traveling through veins is not under pressure from the beating heart. It gets help moving along by the squeezing action of skeletal muscles, for example, when you walk or breathe. It is also prevented from flowing backward by valves in the larger veins, as illustrated in Figure 11.3. and as seen in the ultrasonography image in Figure 11.4. Veins are called capacitance blood vessels, because the majority of the body’s total volume of blood (about 60 per cent) is contained within veins.
Figure 11.3 The two flaps that make up a venous valve can open in just one direction, so blood can flow in only one direction through the vein.Figure 11.4 Here you can see the venous valve opening and closing to allow blood to flow closer to the heart with each contraction of the surrounding skeletal muscle.
Most veins carry deoxygenated blood, but there are a few exceptions, including the four pulmonary veins. These veins carry oxygenated blood from the lungs to the heart, which then pumps the blood to the rest of the body. In virtually all other veins, hemoglobin is relatively unsaturated with oxygen (about 75 per cent).
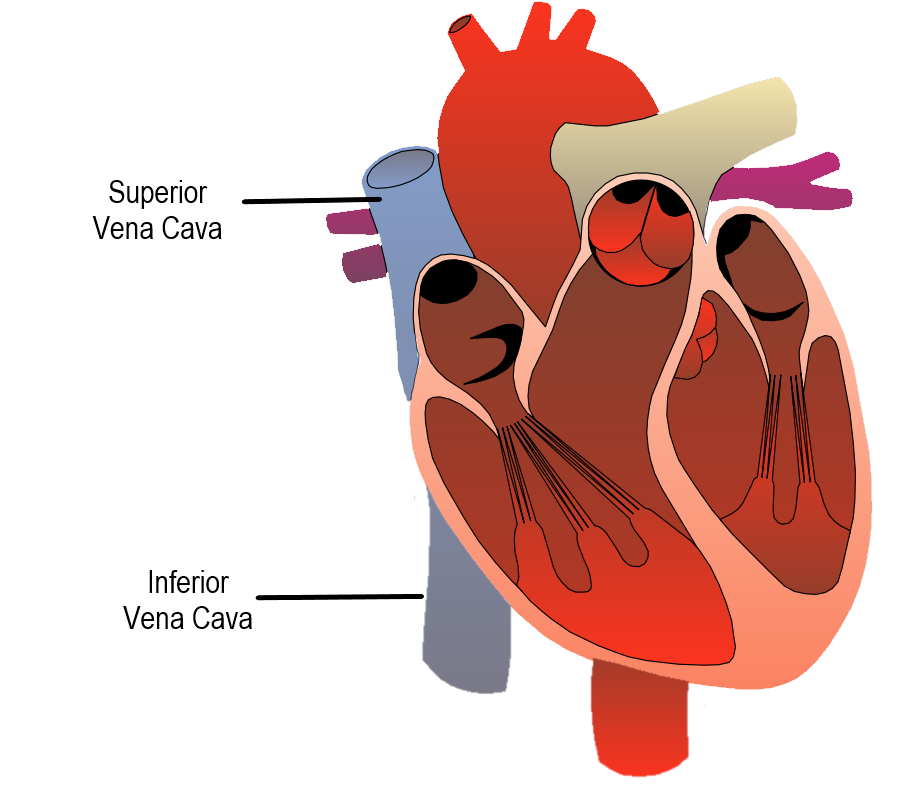
The two largest veins in the body are the superior vena cava — which carries blood from the upper body directly to the right atrium of the heart — and the inferior vena cava, which carries blood from the lower body directly to the right atrium (shown in Figure 11.5). Like arteries, veins form a complex, branching system of larger and smaller vessels. The smallest veins are called venules. They receive blood from capillaries and transport it to larger veins. Each venule receives blood from multiple capillaries.
Figure 11.5 The Superior and Inferior Vena Cava are the largest veins in the body. They deliver deoxygenated blood directly to the right atrium.
CAPILLARIES
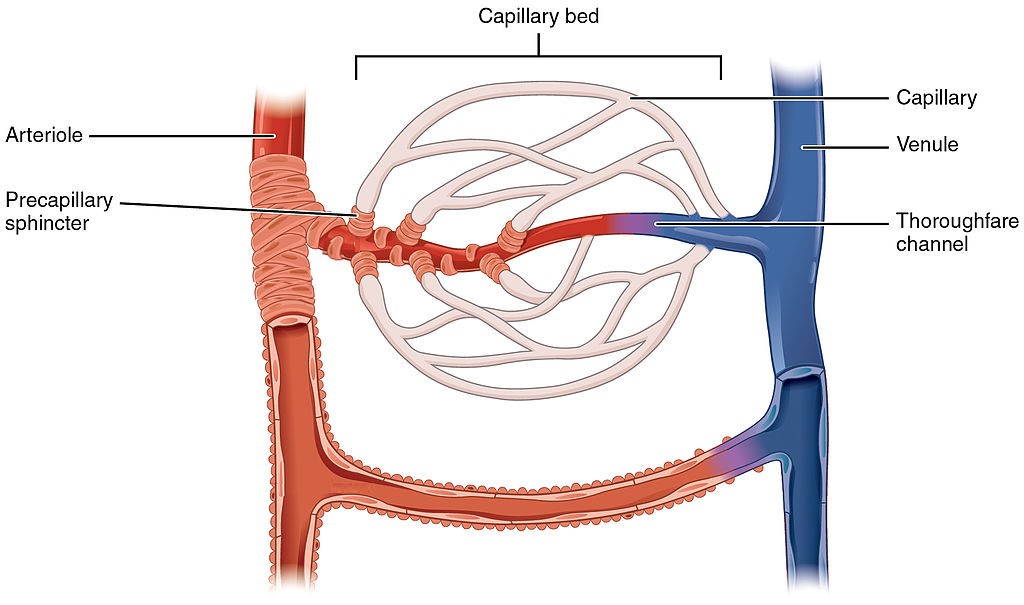
Capillaries are the smallest blood vessels in the cardiovascular system. They are so small that only one red blood cell at a time can squeeze through a capillary, and then only if the red blood cell deforms. Capillaries connect arterioles and venules, as shown in Figure 11.6. Capillaries generally form a branching network of vessels, called a capillary bed, that provides a large surface area for the exchange of substances between the blood and surrounding tissues.
Blood flow through the capillary beds is regulated depending on the body’s needs and is directed by nerve and hormone signals. For example, after a large meal, most of the blood is diverted to the stomach by vasodilation of vessels of the digestive system and vasoconstriction of other vessels. During exercise, blood is diverted to the skeletal muscles through vasodilation while blood to the digestive system would be lessened through vasoconstriction. The blood entering some capillary beds is controlled by small muscles, called precapillary sphincters, illustrated in Figure 11.6. If the sphincters are open, the blood will flow into the associated branches of the capillary blood. If all of the sphincters are closed, then the blood will flow directly from the arteriole to the venule through the thoroughfare channel). These muscles allow the body to precisely control when capillary beds receive blood flow. At any given moment only about 5-10% of our capillary beds actually have blood flowing through them.
Proteins and other large solutes cannot leave the capillaries. The loss of the watery plasma creates a hyperosmotic solution within the capillaries, especially near the venules. This causes about 85% of the plasma that leaves the capillaries to eventually diffuses back into the capillaries near the venules. The remaining 15% of blood plasma drains out from the interstitial fluid into nearby lymphatic vessels (Figure 11.7). The fluid in the lymph is similar in composition to the interstitial fluid. The lymph fluid passes through lymph nodes before it returns to the heart via the vena cava. Lymph nodes are specialized organs that filter the lymph by percolation through a maze of connective tissue filled with white blood cells. The white blood cells remove infectious agents, such as bacteria and viruses, to clean the lymph before it returns to the bloodstream. After it is cleaned, the lymph returns to the heart by the action of smooth muscle pumping, skeletal muscle action, and one-way valves joining the returning blood near the junction of the venae cavae entering the right atrium of the heart.
Figure 11.6 Capillaries form beds of tiny blood vessels that exchange substances with the cells of tissuesFigure 11.7 Fluid from the capillaries moves into the interstitial space and lymph capillaries by diffusion down a pressure gradient and also by osmosis. Out of 7,200 liters of fluid pumped by the average heart in a day, over 1,500 liters is filtered. (credit: modification of work by NCI, NIH) Structure of Blood Vessels
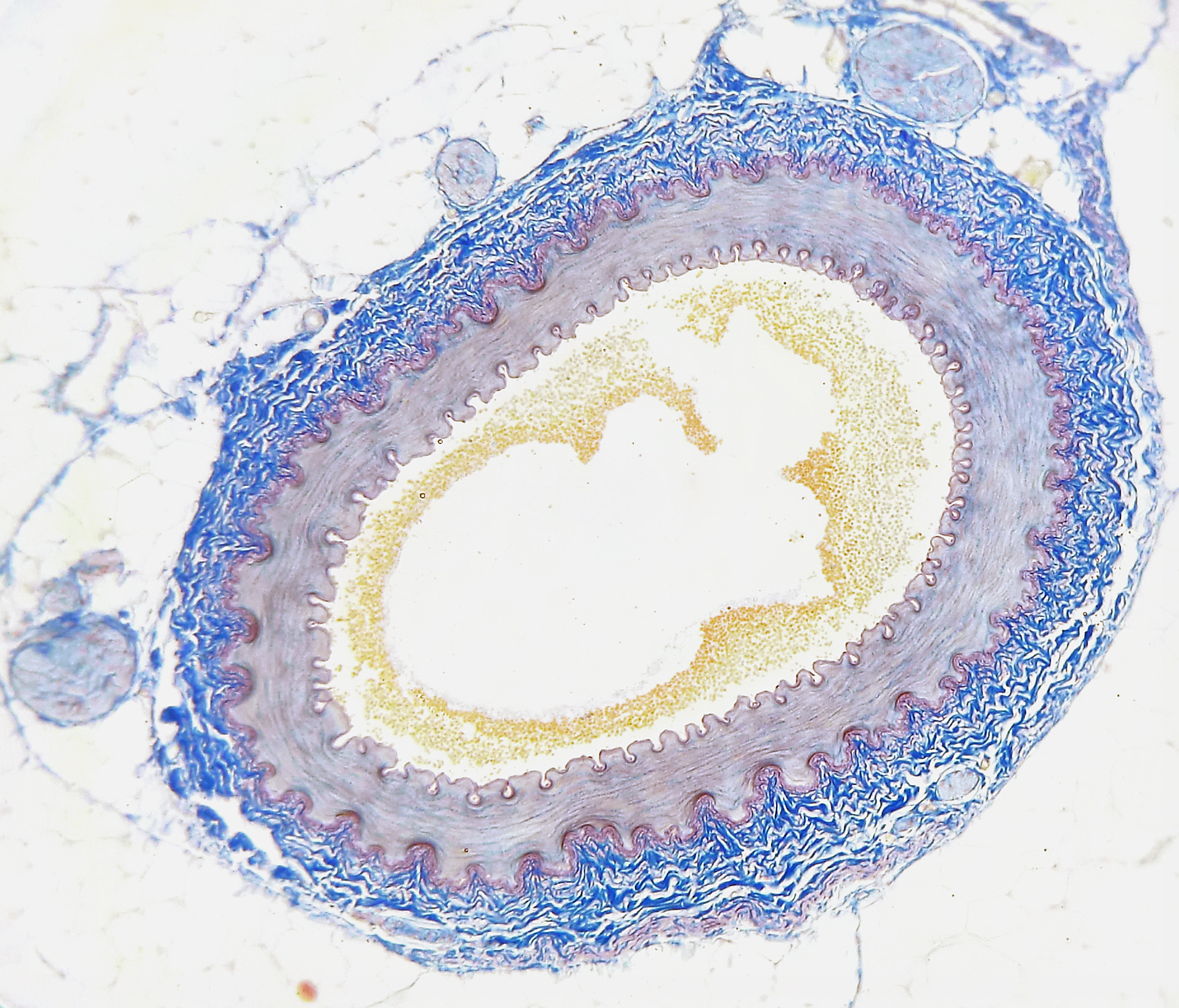
All blood vessels are basically hollow tubes with an internal space, called a lumen, through which blood flows. The lumen of an artery is shown in cross section in the photomicrograph (Figure 11.8). The width of blood vessels varies, but they all have a lumen. The walls of blood vessels differ depending on the type of vessel. In general, arteries and veins are more similar to one another than to capillaries in the structure of their walls.
Figure 11.8 The lumen is the white space in the center of this cross-sectional slice of an artery. You can see that the walls of the artery have multiple layers.
Figure 11.9 Arteries and veins consist of three layers: an outer tunica externa, a middle tunica media, and an inner tunica intima. Capillaries consist of a single layer of epithelial cells, the tunica intima. (credit: modification of work by NCI, NIH)
WALLS OF ARTERIES AND VEINS
The walls of both arteries and veins have three layers (Figure 11.9 above).
Inner layer of arteries and veins (Tunica intima). It is also the thinnest layer, consisting of a single layer of endothelial cells surrounded by a thin layer of connective tissues. It reduces friction between the blood and the inside of the blood vessel walls.
Middle layer of arteries and veins (Tunica media0. In arteries, this is the thickest layer. It consists mainly of elastic fibers and connective tissues. In arteries, this is the thickest layer, because it also contains smooth muscle tissues, which control the diameter of the vessels- as such, the width of this layer can be helpful in distinguishing arteries from veins.
Outer layer of arteries and veins (Tunica externa). It consists of connective tissue, and also contains nerves. In veins, this is the thickest layer. In general, this layer protects and strengthens vessels and attaches them to surrounding structures.
CAPILLARY WALLS
The walls of capillaries consist of little more than a single layer of epithelial cells. Being just one cell thick, the walls are well-suited for the exchange of substances between the blood inside them and the cells of surrounding tissues. Substances including water, oxygen, glucose, and other nutrients, as well as waste products (such as carbon dioxide), can pass quickly and easily through the extremely thin walls of capillaries. See figure 11.10 for a comparison of the structure of arteries, veins and capillaries.
Figure 11.10 There are significant structural differences between arteries, veins and capillaries.
VASOCONSTRICTION AND VASODILATION
Smooth muscles in the walls of arteries can contract or relax to cause vasoconstriction (narrowing of the lumen of blood vessels) or vasodilation (widening of the lumen of blood vessels). This allows the arteries — especially the arterioles — to contract or relax as needed to help regulate blood pressure. In this regard, the arterioles act like an adjustable nozzle on a garden hose. When they narrow, the increased friction with the arterial walls causes less blood to flow downstream from the narrowing, resulting in a drop in blood pressure. These actions are controlled by the autonomic nervous system in response to pressure-sensitive sensory receptors in the walls of larger arteries.
Arteries can also dilate or constrict to help regulate body temperature, by allowing more or less blood to flow from the warm body core to the body’s surface. In addition, vasoconstriction and vasodilation play roles in the fight-or-flight response, under control of the sympathetic nervous system. Vasodilation allows more blood to flow to skeletal muscles, and vasoconstriction reduces blood flow to digestive organs.
Arteries vs Veins (Circulatory System), MooMooMath and Science, 2018.
Review
What are blood vessels? Name the three major types of blood vessels. Compare and contrast how blood moves through arteries and veins. What are capillaries, and what is their function? Does the blood in most veins have any oxygen at all? Explain your answer. Explain why it is important that the walls of capillaries are very thin. What is the role of the lymph capillaries? What is the difference between vasoconstriction and vasodilation? Which of the following best describes veins?
a. thick walled, small lumens, low pressure, lack valves b. thin walled, large lumens, low pressure, have valves c. thin walled, small lumens, high pressure, have valves d. thick walled, large lumens, high pressure, lack valves
11.4 HEART
Figure 11.11 Healthy hearts are happy hearts. What do you hear?
LUB, DUB
Lub dub, lub dub, lub dub… That’s how the sound of a beating heart is typically described. Those are also the only two sounds that should be audible when listening to a normal, healthy heart through a stethoscope, as in Figure 11.11. If a doctor hears something different from the normal lub dub sounds, it’s a sign of a possible heart abnormality. What causes the heart to produce the characteristic lub dub sounds? Read on to find out.
INTRODUCTION TO THE HEART
The heart is a muscular organ behind the sternum (breastbone), slightly to the left of the center of the chest. A normal adult heart is about the size of a fist. The function of the heart is to pump blood through blood vessels of the cardiovascular system. The continuous flow of blood through the system is necessary to provide all the cells of the body with oxygen and nutrients, and to remove their metabolic wastes.
Figure 11.12 The right side of the heart includes the right atrium and right ventricle. The left side includes the left atrium and left ventricle.
As you may have noticed, the Figure 11.11 diagram labels the right side of the heart on the left side of the diagram, and vice versa. This is because it is assumed that in this diagram, the heart appears as if the patient was facing us – the patient’s left side is on our right side!
Unlike skeletal muscle, cardiac muscle routinely contracts without stimulation by the nervous system. Specialized cardiac muscle cells send out electrical impulses that stimulate the contractions. As a result, the atria and ventricles normally contract with just the right timing to keep blood pumping efficiently through the heart.
STRUCTURE OF THE HEART
The heart has a thick muscular wall that consists of several layers of tissue. Internally, the heart is divided into four chambers through which blood flows. Because of heart valves, blood flows in just one direction through the chambers.
HEART WALL
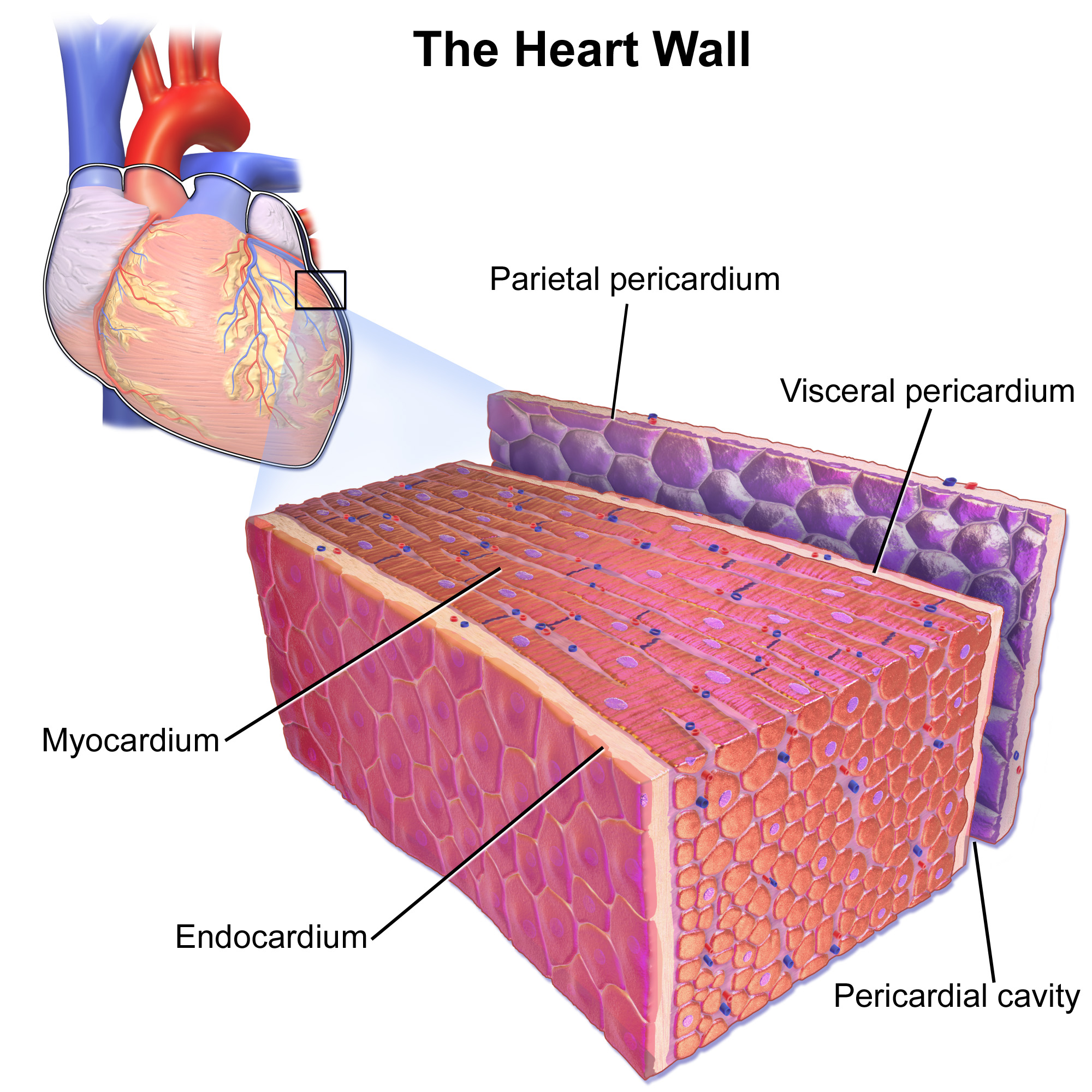
Figure 11.13 The wall of the heart is made up mainly of myocardium, which consists largely of cardiac muscle.As shown in Figure 11.13, the wall of the heart is made up of three layers, called the endocardium, myocardium, and pericardium.
The endocardium is the innermost layer of the heart wall. It is made up primarily of simple epithelial cells. It covers the heart chambers and valves. A thin layer of connective tissue joins the endocardium to the myocardium.
The myocardium is the middle and thickest layer of the heart wall. It consists of cardiac muscle surrounded by a framework of collagen. There are two types of cardiac muscle cells in the myocardium: cardiomyocytes — which have the ability to contract easily — and pacemaker cells, which conduct electrical impulses that cause the cardiomyocytes to contract. About 99 per cent of cardiac muscle cells are cardiomyocytes, and the remaining one per cent is pacemaker cells. The myocardium is supplied with blood vessels and nerve fibers via the pericardium.
The pericardium is a protective sac that encloses and protects the heart. The pericardium consists of two membranes (visceral pericardium and parietal pericardium), between which there is a fluid-filled cavity. The fluid helps to cushion the heart, and also lubricates its outer surface.
HEART CHAMBERS
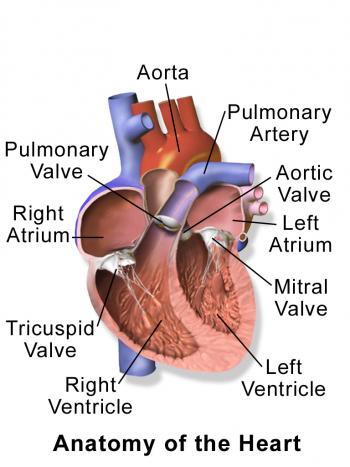
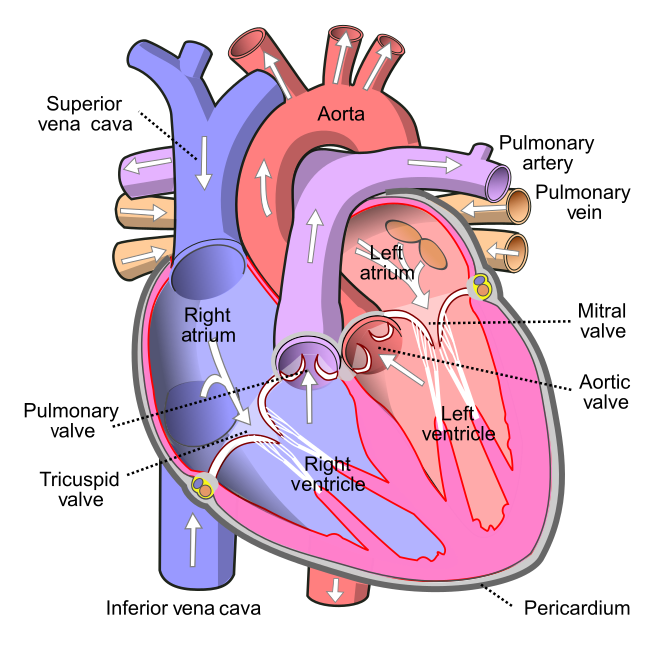
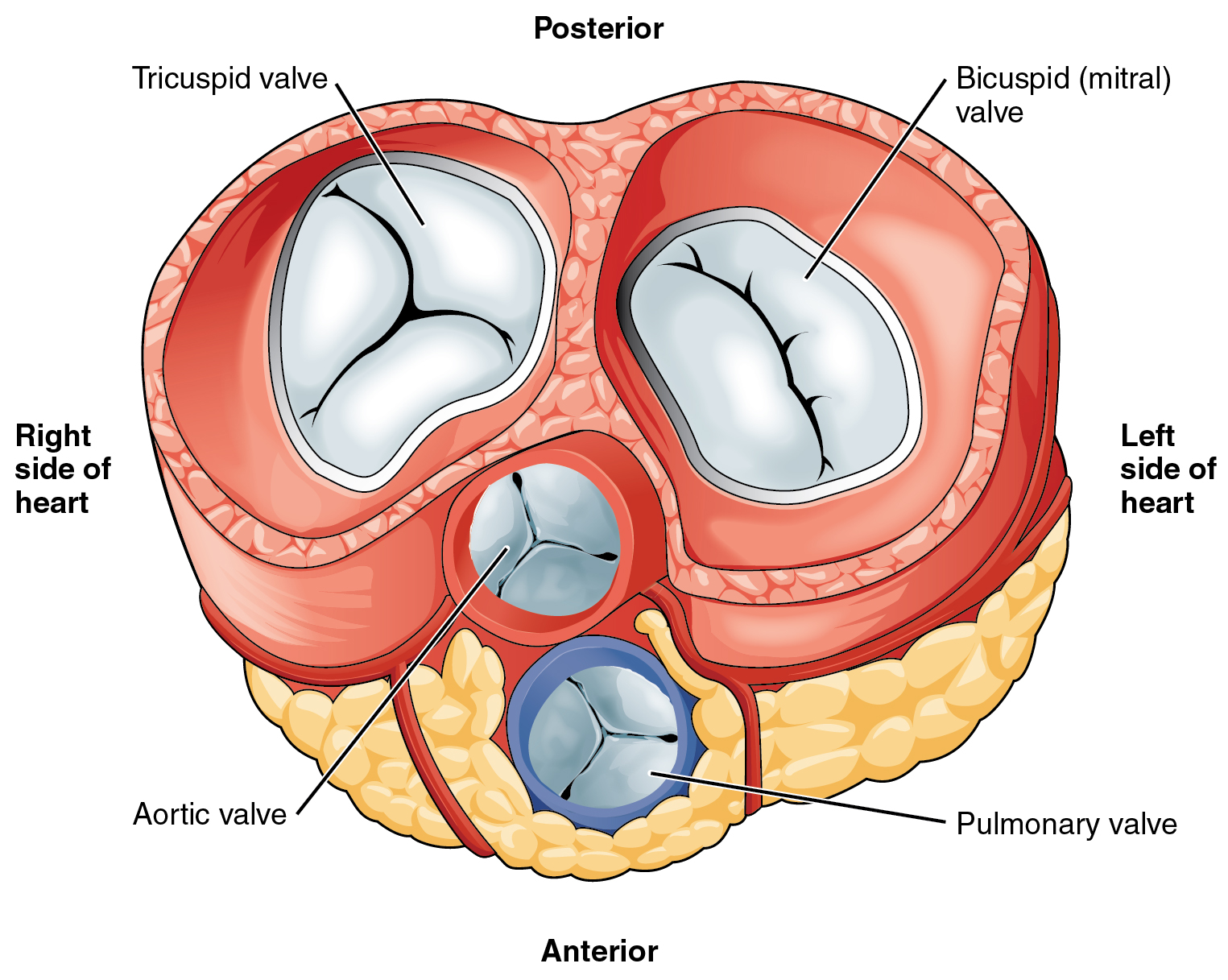
As shown in Figure 11.14 the four chambers of the heart include two upper chambers called atria (singular, atrium), and two lower chambers called ventricles. The atria are also referred to as receiving chambers, because blood coming into the heart first enters these two chambers. The right atrium receives deoxygenated blood from the upper and lower body through the superior vena cava and inferior vena cava, respectively. The left atrium receives oxygenated blood from the lungs through the pulmonary veins. The ventricles are also referred to as discharging chambers, because blood leaving the heart passes out through these two chambers. The right ventricle discharges blood to the lungs through the pulmonary artery, and the left ventricle discharges blood to the rest of the body through the aorta. The four chambers are separated from each other by dense connective tissue consisting mainly of collagen. Figure 11.14 This cross-sectional diagram of the heart shows its four chambers and four valves. The white arrows indicate the direction of blood flow through the heart chambers.HEART VALVES Figure 11.15 If the veins and arteries of the heart were removed, a top-down view of the heart would reveal the four valves that are critical in preventing backflow of blood. Note the three cusps of the tricuspid AV valve and the 2 cusps of the bicuspid AV valve. Also note the size difference between the AV valves and the semilunar valves.
Figure 11.15 shows the location of the heart’s four valves in a top-down view, looking down at the heart as if the arteries and veins feeding into and out of the heart were removed. The heart valves allow blood to flow from the atria to the ventricles, and from the ventricles to the pulmonary artery and aorta. The valves are constructed in such a way that blood can flow through them in only one direction, thus preventing the backflow of blood. Figure 11.15 shows how valves open to let blood into the appropriate chamber, and then close to prevent blood from moving in the wrong direction and the next chamber contracts. The four valves are the:
Tricuspid atrioventricular valve, (can be shortened to tricuspid AV valve) which allows blood to flow from the right atrium to the right ventricle. Bicuspid atrioventricular valve(also known as the mitral valve), which allows blood to flow from the left atrium to the left ventricle. Pulmonary semilunar valve, which allows blood to flow from the right ventricle to the pulmonary artery. Aortic semilunar valve, which allows blood to flow from the left ventricle to the aorta.
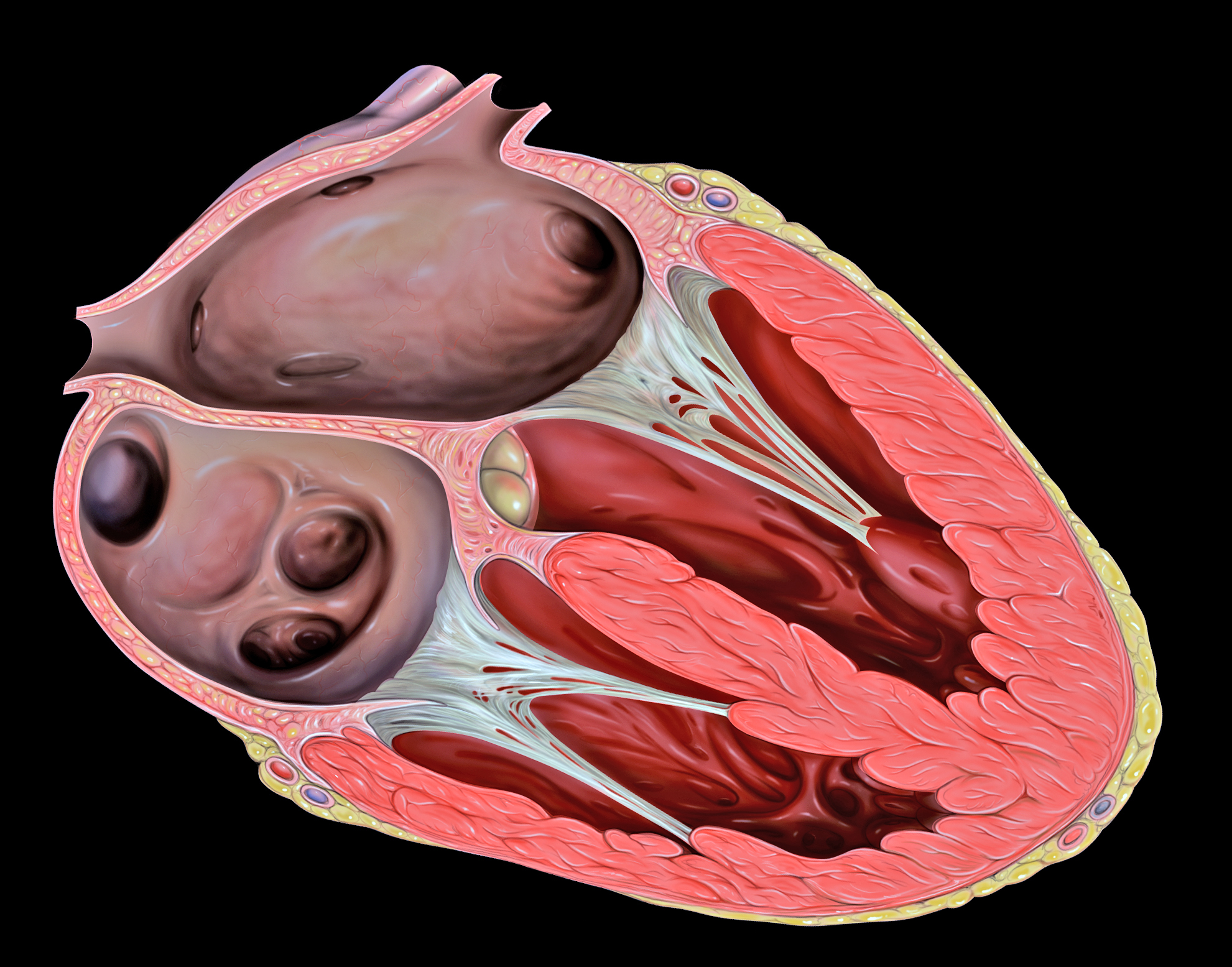
Figure 11.16 The valves of the heart prevent backflow of blood. The open when the chamber before them contracts (systole) and then close when that chamber relaxes (diastole).Figure 11.17 The chordae tendineae, shown in this diagram in white, play a critical role in reinforcing the AV valves of the heart.The two atrioventricular (AV) valves prevent backflow when the ventricles are contracting, while the semilunar valves prevent backflow from vessels. This means that the AV valves must withstand much more pressure than do the semilunar valves. In order to withstand the force of the ventricles contracting (to prevent blood from backflowing into the atria), the AV valves are reinforced with structures called chordae tendineae — tendon-like cords of connective tissue which anchor the valve and prevent it from prolapse. Figure 11.17 shows the structure and location of the chordae tendineae.
The chordae tendineae are under such force that they need special attachments to the interior of the ventricles where they anchor. Papillary muscles are specialized muscles in the interior of the ventricle that provide a strong anchor point for the chordae tendineae. CORONARY CIRCULATION
The cardiomyocytes of the muscular walls of the heart are very active cells, because they are responsible for the constant beating of the heart. These cells need a continuous supply of oxygen and nutrients. The carbon dioxide and waste products they produce also must be continuously removed. The blood vessels that carry blood to and from the heart muscle cells make up the coronary circulation. Note that the blood vessels of the coronary circulation supply heart tissues with blood, and are different from the blood vessels that carry blood to and from the chambers of the heart as part of the general circulation. Coronary arteriessupply oxygen-rich blood to the heart muscle cells. Coronary veins remove deoxygenated blood from the heart muscles cells.
There are two coronary arteries — a right coronary artery that supplies the right side of the heart, and a left coronary artery that supplies the left side of the heart. These arteries branch repeatedly into smaller and smaller arteries and finally into capillaries, which exchange gases, nutrients, and waste products with cardiomyocytes.
At the back of the heart, small cardiac veins drain into larger veins, and finally into the great cardiac vein, which empties into the right atrium. At the front of the heart, small cardiac veins drain directly into the right atrium.
TWO CIRCULATIONS
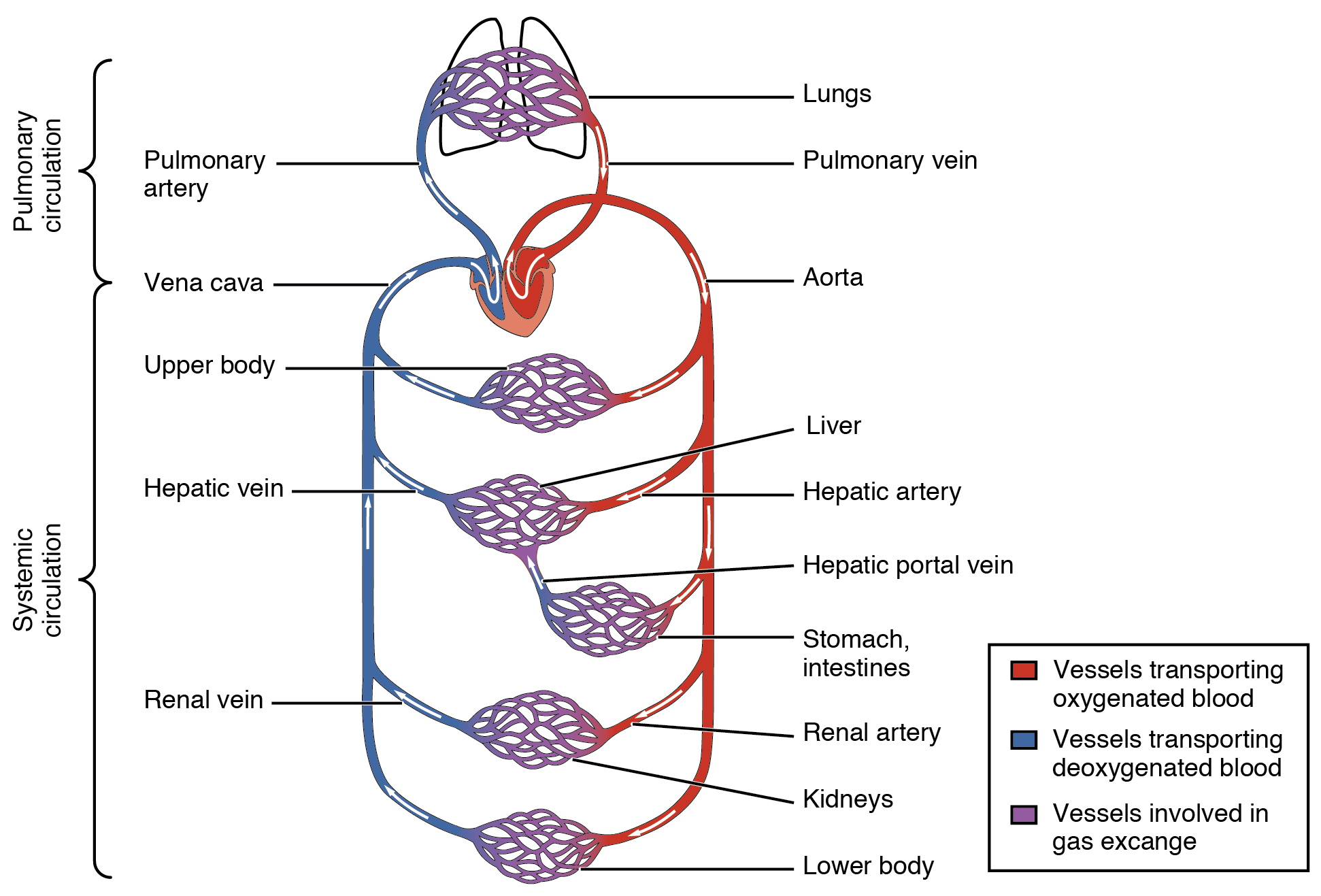
Cells throughout the body need a constant supply of oxygen. They get oxygen from capillaries in the systemic circulation. The systemic circulation is just one of two interconnected circulations that make up the human cardiovascular system. The other circulation is the pulmonary system, which is where blood picks up oxygen to carry to cells. It takes blood about 20 seconds to make one complete transit through both circulations (see Figure 11.18).
Figure 11.18 There are two main circuits through which blood flows in the cardiovascular system. In the pulmonary circuit, blood moves from the right side of the heart to the lungs and then back to the left side of the heart. In the systemic circuit, blood moves from the left side of the heart to the body tissues and then back to the right side of the heart.PULMONARY CIRCUIT
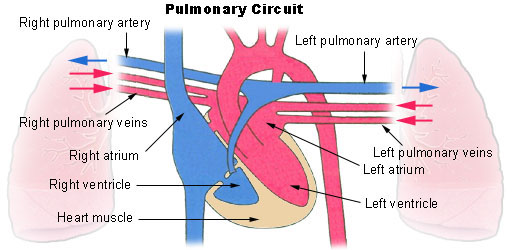
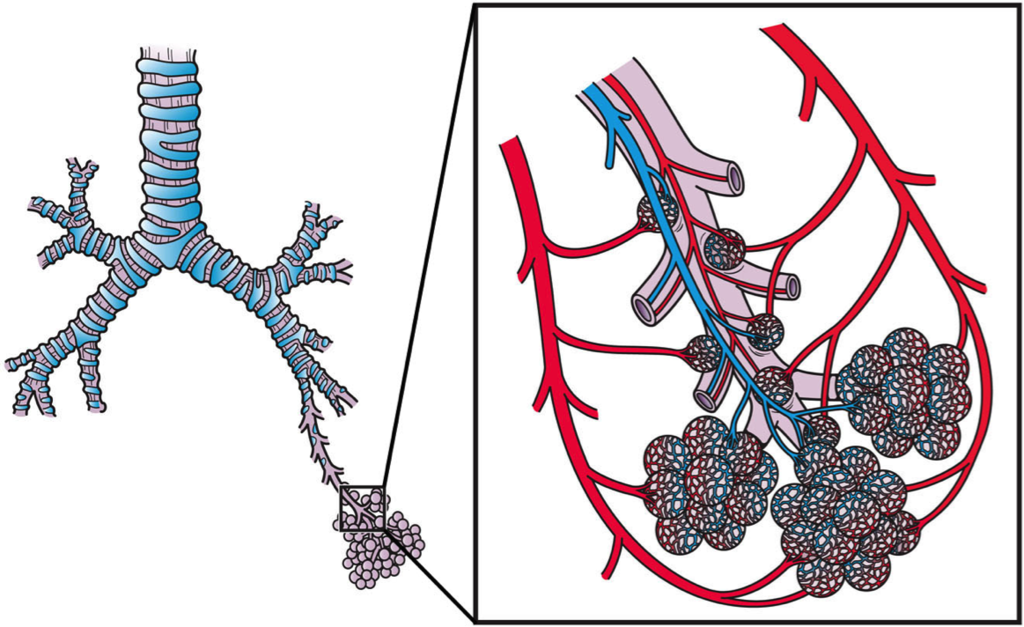
The pulmonarycircuit involves only the heart, the lungs, and the major blood vessels that connect them (illustrated in Figure 11.19). Blood moves through the pulmonary circuit from the heart to the lungs, and then back to the heart again, becoming oxygenated in the process. Specifically, the right ventricle of the heart pumps deoxygenated blood into the right and left pulmonary arteries. These arteries carry the blood to the right and left lungs, respectively. Oxygenated blood then returns from the right and left lungs through the two right and two left pulmonary veins. All four pulmonary veins enter the left atrium of the heart. Figure 11.19 This diagram shows the heart, lungs, and major vessels that make up the pulmonary circulation. The colored arrows indicate the direction of blood flow — red for oxygenated blood and blue for relatively deoxygenated blood.What happens to the blood while it is in the lungs? It passes through increasingly smaller arteries, and finally through capillary networks surrounding the alveoli (see Figure 11.20). This is where gas exchange takes place. The deoxygenated blood in the capillaries picks up oxygen from the alveoli and gives up carbon dioxide to the alveoli. As a result, the blood returning to the heart in the pulmonary veins is almost completely saturated with oxygen. Figure 11.20 This diagram illustrates clusters of alveoli in the lungs, where gas exchange takes place with blood in capillaries as it passes through the pulmonary circulation.SYSTEMIC CIRCULATION
The oxygenated blood that enters the left atrium of the heart in the pulmonary circulation then passes into the systemic circuit. This is the part of the cardiovascular system that transports blood to and from all of the tissues of the body to provide oxygen and nutrients, and to pick up wastes. It consists of the heart and blood vessels that supply the metabolic needs of all the cells in the body, including those of the heart and lungs.
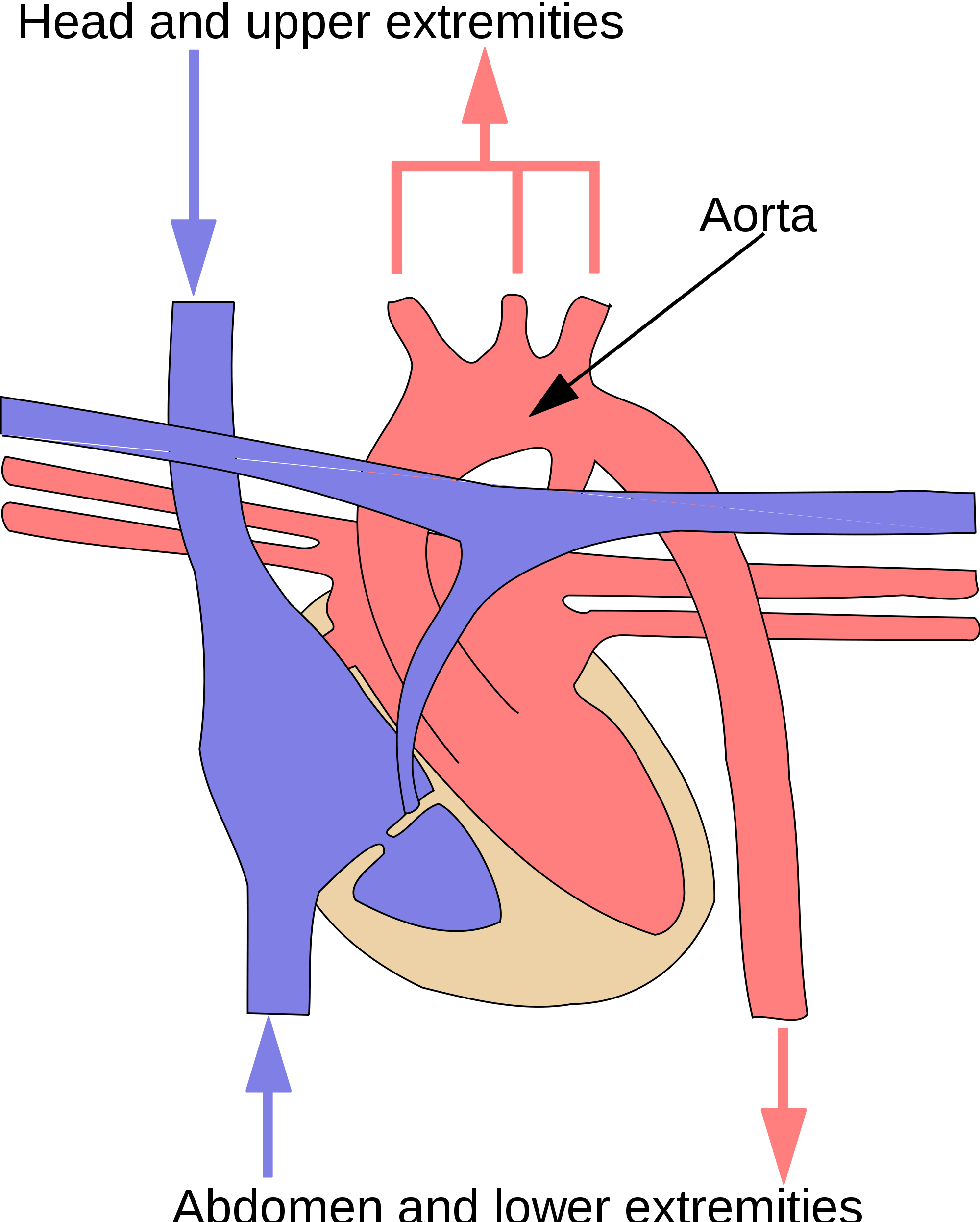
As shown in Figure 11.21, in the systemic circulation, the left atrium pumps oxygenated blood to the left ventricle, which pumps the blood directly into the aorta, the body’s largest artery. Major arteries branching off the aorta carry the blood to the head and upper extremities. The aorta continues down through the abdomen and carries blood to the abdomen and lower extremities. The blood then returns to the heart through the network of increasingly larger veins of the systemic circulation. All of the returning blood eventually collects in the superior vena cava (upper body) and inferior vena cava (lower body), which empty directly into the right atrium of the heart. Figure 11.21 The systemic circulation includes the aorta (red), which carries oxygenated blood away from the heart to the rest of the body; and the inferior and superior venae cavae (blue), which return deoxygenated blood to the heart from the body. The colored arrows in the diagram indicate the direction of blood flow — red for oxygenated and blue for deoxygenated.BLOOD CIRCULATION THROUGH THE HEART
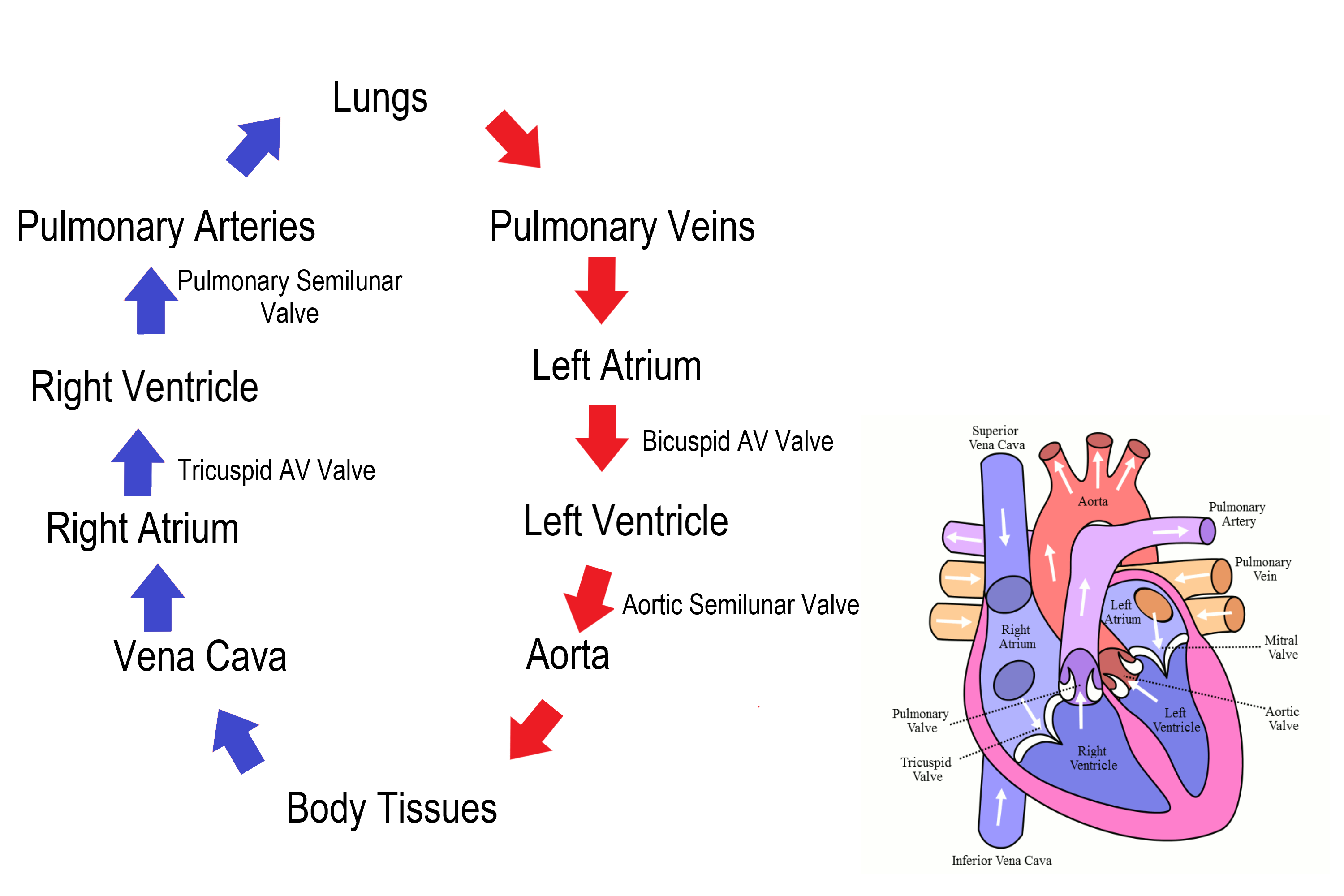
Figure 11.22 shows how blood circulates through the chambers of the heart. The right atrium collects blood from two large veins, the superior vena cava (from the upper body) and the inferior vena cava (from the lower body). The blood that collects in the right atrium is pumped through the tricuspid valve into the right ventricle. From the right ventricle, the blood is pumped through the pulmonary valve into the pulmonary artery. The pulmonary artery carries the blood to the lungs, where it enters the pulmonary circulation, gives up carbon dioxide, and picks up oxygen. The oxygenated blood travels back from the lungs through the pulmonary veins (of which there are four) and enters the left atrium of the heart. From the left atrium, the blood is pumped through the mitral valve into the left ventricle. From the left ventricle, the blood is pumped through the aortic valve into the aorta, which subsequently branches into smaller arteries that carry the blood throughout the rest of the body. After passing through capillaries and exchanging substances with cells, the blood returns to the right atrium via the superior vena cava and inferior vena cava, and the process begins anew. Figure 11.22The flow chart in this diagram summarizes the pathway blood takes as it flows into, through, and out of the heart. Trace the path of blood flow in the diagram of the heart as you follow it through the flow chart.CARDIAC CYCLE
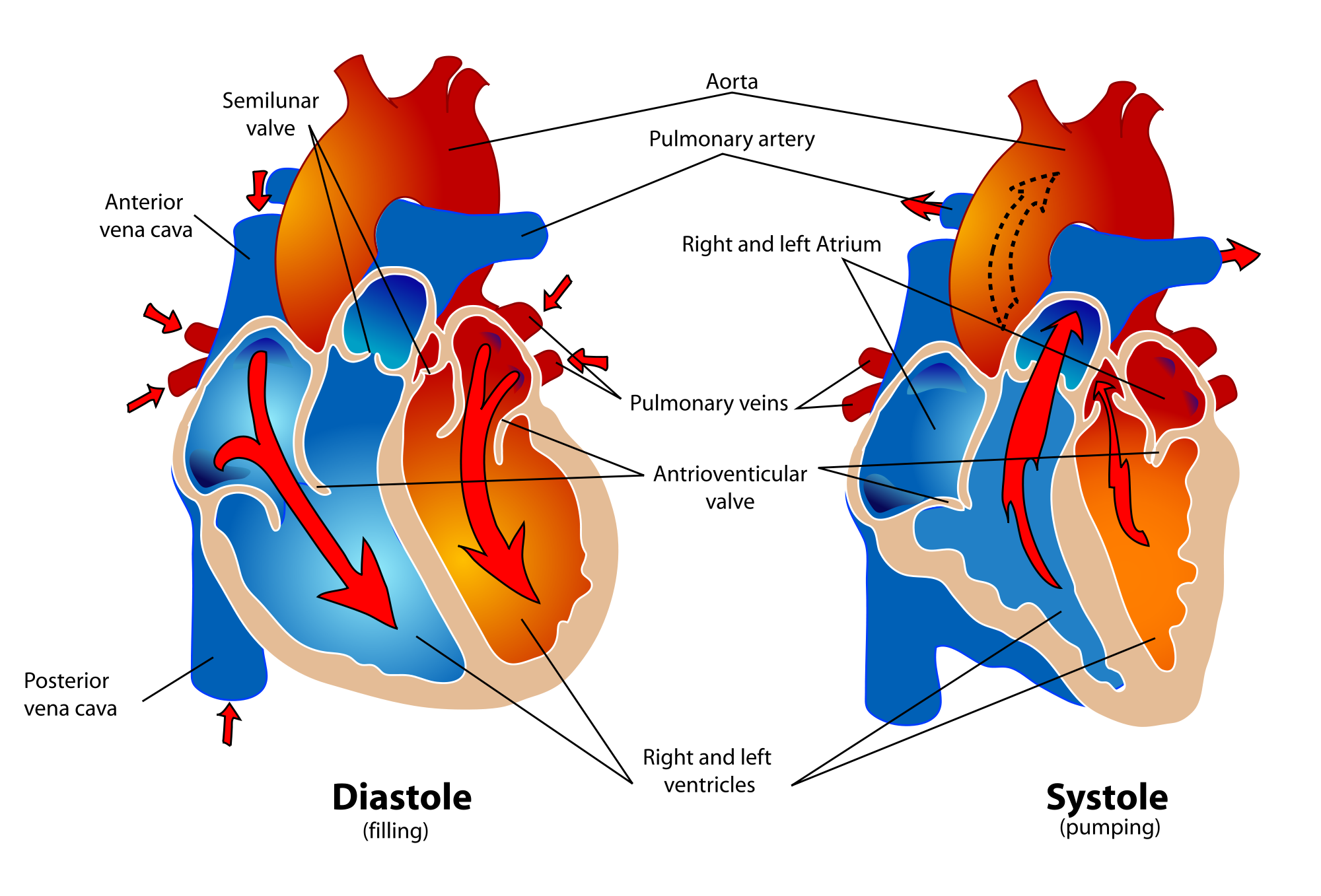
The cardiac cycle refers to a single complete heartbeat, which includes one iteration of the lub and dub sounds heard through a stethoscope. During the cardiac cycle, the atria and ventricles work in a coordinated fashion so that blood is pumped efficiently through and out of the heart. The cardiac cycle includes two parts, called diastole and systole, which are illustrated in the diagrams in Figure 11.23.
During diastole, the atria contract and pump blood into the ventricles, while the ventricles relax and fill with blood from the atria.
During systole, the atria relax and collect blood from the lungs and body, while the ventricles contract and pump blood out of the heart.
Figure 11.23 Diastole is referred to the filling stage, because this is when the ventricles fill with blood. Systole is referred to the pumping stage because this is when the ventricles pump blood out of the heart.Electrical Stimulation of the Heart
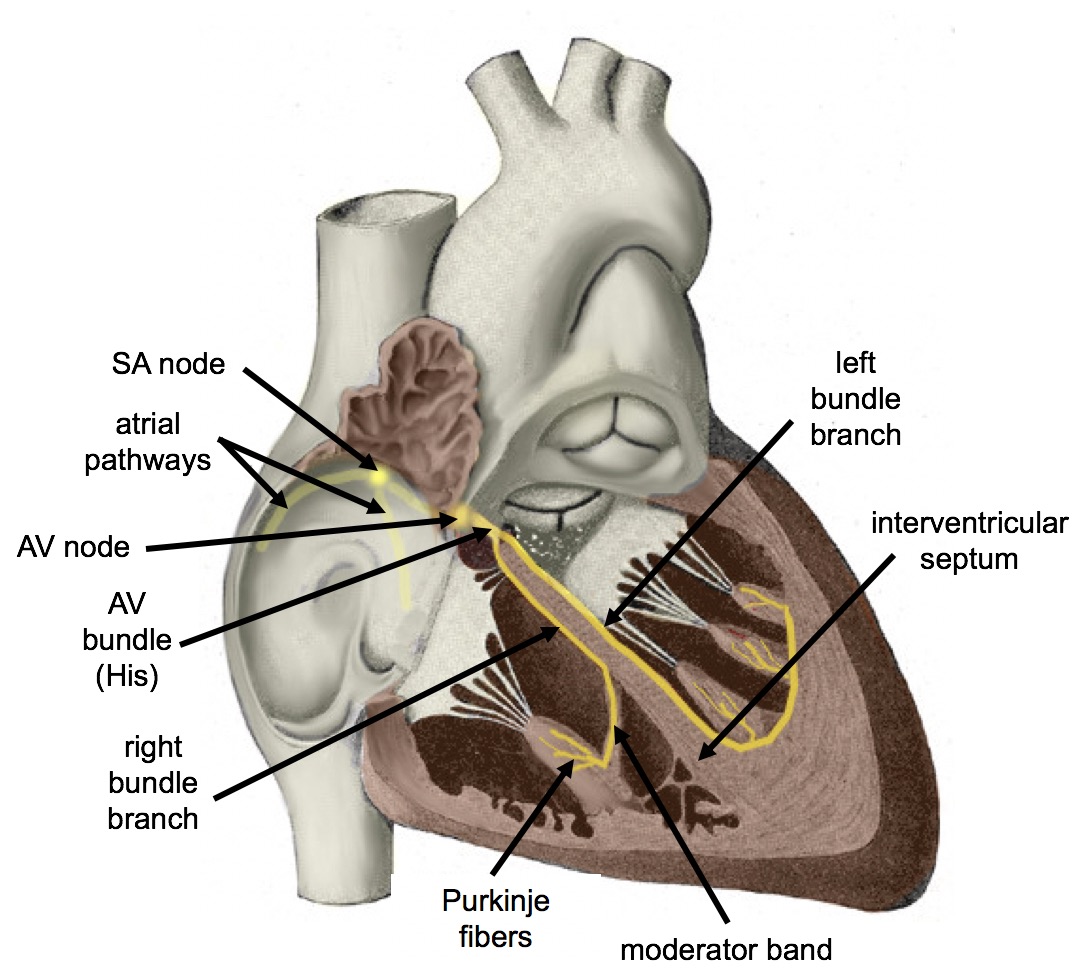
The normal, rhythmical beating of the heart is called sinus rhythm. It is established by the heart’s pacemaker cells, which are located in an area of the heart called the sinoatrial node (shown in Figure 11.23). The pacemaker cells create electrical signals with the movement of electrolytes (sodium, potassium, and calcium ions) into and out of the cells. For each cardiac cycle, an electrical signal rapidly travels first from the sinoatrial node to the right and left atria, so they contract together. Then, the signal travels to another node, called the atrioventricular node (Figure 11.24), and from there to the right and left ventricles (which also contract together), just a split second after the atria contract. Figure 11.24 The sinoatrial (SA) node causes the atria to contract and then signals the atrioventricular (AV) nodes to initiate the contraction of the ventricles.The normal sinus rhythm of the heart is influenced by the autonomic nervous system through sympathetic and parasympathetic nerves. These nerves arise from two paired cardiovascular centers in the medulla of the brainstem. The parasympathetic nerves act to decrease the heart rate, and the sympathetic nerves act to increase the heart rate. Parasympathetic input normally predominates. Without it, the pacemaker cells of the heart would generate a resting heart rate of about 100 beats per minute, instead of a normal resting heart rate of about 72 beats per minute. The cardiovascular centers receive input from receptors throughout the body, and act through the sympathetic nerves to increase the heart rate, as needed. Increased physical activity, for example, is detected by receptors in muscles, joints, and tendons. These receptors send nerve impulses to the cardiovascular centers, causing sympathetic nerves to increase the heart rate, and allowing more blood to flow to the muscles.
Besides the autonomic nervous system, other factors can also affect the heart rate. For example, thyroid hormones and adrenal hormones (such as epinephrine) can stimulate the heart to beat faster. The heart rate also increases when blood pressure drops or the body is dehydrated or overheated. On the other hand, cooling of the body and relaxation — among other factors — can contribute to a decrease in the heart rate.
Electrocardiogram (ECG or EKG)
What is an EKG?
An electrocardiogram — abbreviated as EKG or ECG — measures the electrical activity of the heartbeat. With each beat, an electrical impulse (or “wave”) travels through the heart. This electrical wave causes the muscle to squeeze and pump blood from the heart. A normal heartbeat on ECG will show the rate and rhythm of the contractions in the upper and lower chambers.
The right and left atria or upper chambers make the first wave called a “P wave” — following a flat line when the electrical impulse goes to the bottom chambers or ventricles. The right and left bottom chambers make the next wave called a “QRS complex.” The final wave, or “T wave,” represents electrical recovery or return to a resting state for the ventricles.
Figure 11.25 EKG strip showing a normal heartbeat
Review
What is the heart, where is located, and what is its function?
Describe the walls of the heart.
Describe the coronary circulation.
Summarize how blood flows into, through, and out of the heart.
Explain what controls the beating of the heart.
Explain why the blood from the cardiac veins empties into the right atrium of the heart. Focus on function (rather than anatomy) in your answer.
What are the four chambers of the heart?
What are the four valves of the heart?
What is the difference between pulmonary and systemic circulations?
Describe the electrical activity of the heart.
What is an EKG?
11.5 BLOOD PRESSURE
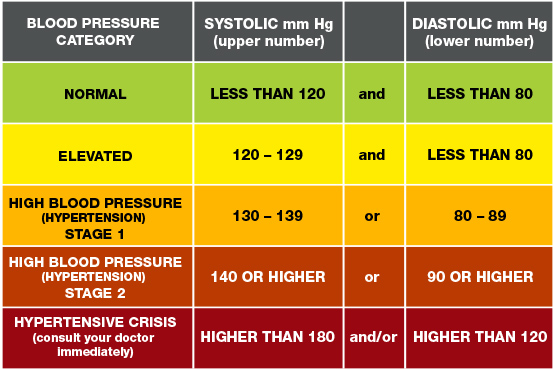
The blood in arteries is normally under pressure because of the beating of the heart. The pressure is highest when the heart contracts and pumps out blood, and lowest when the heart relaxes and refills with blood. (You can feel this variation in pressure in your wrist or neck when you count your pulse.) Blood Pressure is a measure of the force that blood exerts on the walls of arteries. It is generally measured in millimeters of mercury (mm Hg) and expressed as a double number — a higher number for systolic pressure when the ventricles contract, and a lower number for diastolic pressure when the ventricles relax. Normal blood pressure is generally defined as less than 120 mm Hg (systolic)/80 mm Hg (diastolic) when measured in the arm at the level of the heart. It decreases as blood flows farther away from the heart and into smaller arteries. As arteries grow smaller, there is increasing resistance to blood flow through them, because of the blood’s friction against the arterial walls. This resistance restricts blood flow so that less blood reaches smaller, downstream vessels, thus reducing blood pressure before the blood flows into the tiniest vessels, the capillaries. Without this reduction in blood pressure, capillaries would not be able to withstand the pressure of the blood without bursting. By the time blood flows through the veins, it is under very little pressure. The pressure of blood against the walls of veins is always about the same — normally no more than 10 mm Hg.
During systole, when new blood is entering the arteries, the artery walls stretch to accommodate the increase of pressure of the extra blood; during diastole, the walls return to normal because of their elastic properties. The blood pressure of the systole phase and the diastole phase, graphed in Figure 11.26, gives the two pressure readings for blood pressure. For example, 120/80 indicates a reading of 120 mm Hg during the systole and 80 mm Hg during diastole. Throughout the cardiac cycle, the blood continues to empty into the arterioles at a relatively even rate. Figure 11.26 Blood pressure is related to the blood velocity in the arteries and arterioles. In the capillaries and veins, the blood pressure continues to decease but velocity increases.
How blood pressure works – Wilfred Manzano, TED-Ed, 2015.
Review
What is blood pressure?
What is the difference between systolic and diastolic pressures?
11.6 Blood Pressure Regulation
Cardiac output is the volume of blood pumped by the heart in one minute. It is calculated by multiplying the number of heart contractions that occur per minute (heart rate) times the stroke volume (the volume of blood pumped into the aorta per contraction of the left ventricle). Therefore, cardiac output can be increased by increasing heart rate, as when exercising. However, cardiac output can also be increased by increasing stroke volume, such as if the heart contracts with greater strength. Stroke volume can also be increased by speeding blood circulation through the body so that more blood enters the heart between contractions. During heavy exertion, the blood vessels relax and increase in diameter, offsetting the increased heart rate and ensuring adequate oxygenated blood gets to the muscles. Stress triggers a decrease in the diameter of the blood vessels, consequently increasing blood pressure. These changes can also be caused by nerve signals or hormones, and even standing up or lying down can have a great effect on blood pressure.
Thenervoussystem is critical in the role of blood pressure regulation. The medulla oblongata is the primary cardiovascular site of the brain. There are specialized stretch receptors called baroreceptors located within the aorta and carotid arteries that respond to the degree of stretch due to the presence of blood. These receptors send signals to the medulla oblongata to regulate blood pressure.
As blood pressure increases the baroreceptors stretch and send signals to the medulla oblongata. The medulla in turns sends signals to the heart reduces its heart rate and force of contraction. At the same time a signal is transmitted to the arterioles to vasodilate which increases blood flow to the tissues through the parasympathetic nervous system. These two actions lower blood pressure.
To increase blood pressure, the baroreceptors decrease the signals they send. This causes cardiac output to increase and the arterioles vasoconstrict via the sympathetic nervous system. The activities of both results in a higher blood pressure.
11.7 CARDIOVASCULAR DISEASE
Figure 11.27 Why does fat taste so good?
HEART ATTACK ON A PLATE
Eating this greasy cheeseburger smothered in cheese may not literally cause a heart attack — but regularly eating high-fat, low-fiber foods like this may increase the risk of a heart attack, as well as other types of cardiovascular disease. Unhealthy lifestyle choices such as this may actually account for as much as 90% of cardiovascular disease.
WHAT IS CARDIOVASCULAR DISEASE?
Cardiovascular disease is a class of diseases that involve the cardiovascular system. They include diseases of the coronary arteries that supply the heart muscle with oxygen and nutrients, diseases of arteries (such as the carotid artery) that provide blood flow to the brain; and diseases of the peripheral arteries that carry blood throughout the body. Worldwide, cardiovascular disease is the leading cause of death, causing about 1/3 of all deaths each year.
Most cases of cardiovascular disease occur in people over the age of 60, with disease typically setting in about a decade earlier for males than females. You can’t control your age or sex, but you can control other factors that increase the risk of cardiovascular disease. These factors include smoking, obesity, diabetes, high blood levels of cholesterol, and lack of exercise. Most cases of cardiovascular disease can be prevented by controlling these risk factors. Not smoking, maintaining a healthy weight, eating a healthy diet, taking medications as needed to control diabetes and cholesterol, and getting regular exercise are all ways to prevent cardiovascular disease, or to keep it from progressing. It should be noted that although high blood lipid levels are definitely risk factors for cardiovascular disease, the connection between blood lipid levels and fat in the diet is not well understood. For example, high levels of cholesterol in the diet do not appear to lead directly to high levels of cholesterol in the blood. Clearly, cardiovascular disease is multifactorial in terms of its causes.
PRECURSORS OF CARDIOVASCULAR DISEASE
There are two very common conditions that are precursors to virtually all cases of cardiovascular disease: hypertension (or high blood pressure) and atherosclerosis, commonly called hardening of the arteries. Both conditions affect the arteries and their ability to maintain normal blood flow.
What is High Blood Pressure?
High blood pressure is also known as hypertension. It happens when the force of your blood pushing against the walls of your blood vessels is too high. High blood pressure can lead to other serious problems such as heart attack or stroke. When blood pressure is high for too long, it can damage the walls of blood vessels, causing them to develop tiny tears. To fix these damaged areas, the body sends special cells that stick to the site. Over time, substances such as cholesterol and fats may also build up at these damaged spots, forming plaque. As plaque slowly builds, a process called atherosclerosis, it can make the inside of the arteries narrower. This narrowing can block the flow of blood, further increasing blood pressure.
Nearly half of U.S. adults have high blood pressure. Many don’t even know they have it. The only way to know you have high blood pressure is to have your blood pressure checked. A diagnosis of high blood pressure will need to be made by a health care professional.
High blood pressure is classified as either primary or secondary high blood pressure. At least 90% of cases are primary high blood pressure, which is caused by some combination of genetic and lifestyle factors. Numerous genes have been identified as having small effects on blood pressure. Lifestyle factors that increase the risk of high blood pressure include excess dietary salt and alcohol consumption, as well as the risk factors for cardiovascular disease listed above. Secondary high blood pressure, which makes up the remaining ten per cent of cases of hypertension, is attributable to a particular identifiable cause, such as chronic kidney disease or an endocrine disorder (such as Cushing’s disease).
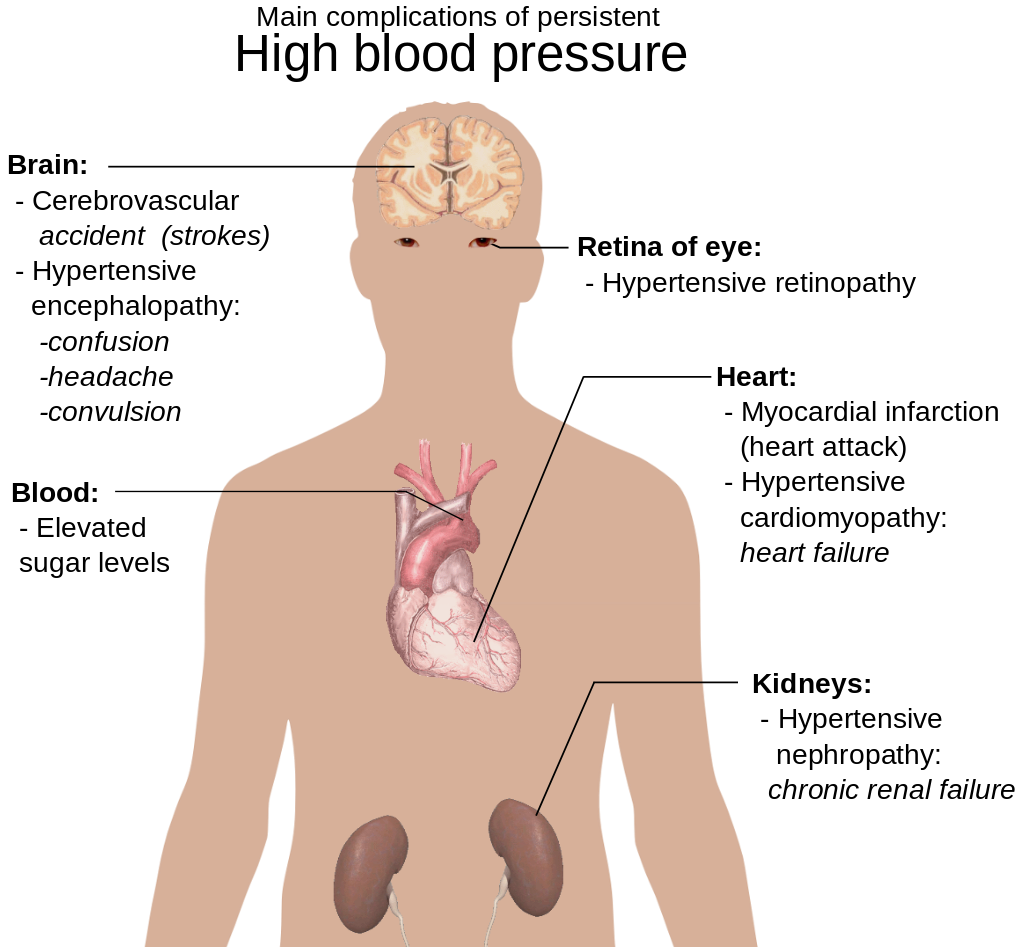
Treating hypertension is important for reducing the risk of all types of cardiovascular disease, especially stroke. These and other complications of persistent high blood pressure are shown in Figure 11.29. Lifestyle changes, such as reducing salt intake and adopting a healthier diet may be all that’s needed to lower blood pressure to the normal range. In many cases, however, medications are also required. The majority of people with high blood pressure have to take more than one medication to fully control their hypertension.
Figure 11.29 If high blood pressure is not brought under control, it can eventually have many detrimental effects.
130 Is Too High for Blood Pressure (American Heart Association)
ATHEROSCLEROSIS
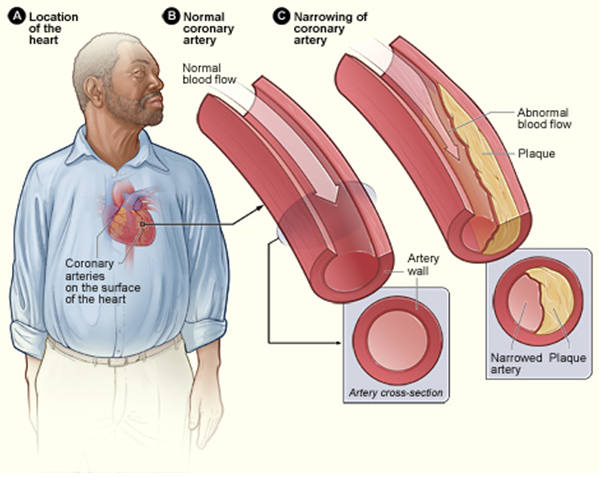
Atherosclerosis is a condition in which artery walls thicken and stiffen as a result of the buildup of plaques inside the arteries, similarly to minerals collecting in plumbing that carries hard water. Plaques consist of leukocytes, cholesterol, and other fats. Typically, there is also a proliferation of smooth muscle cells that make the plaque fibrous, as well as fatty. Over time, the plaques may harden with the addition of calcium crystals. This reduces the elasticity of the artery walls. As plaques increase in size, the artery walls dilate to compensate so blood flow is not affected. Eventually, however, the lumen of the arteries is likely to become so narrowed by plaque buildup that blood flow is reduced, or even blocked entirely. Figure 11.30 illustrates the formation of a plaque in a coronary artery.
Figure 11.30 A plaque in a coronary artery may reduce blood flow to cardiac muscle cells.
In most people, plaques start to form in arteries during childhood, and progress throughout life. Individuals may develop just a few plaques, or dozens of them. Plaques typically remain asymptomatic for decades. Signs and symptoms appear only after there is severe narrowing (stenosis) or complete blockage of arteries. As plaques increase in size and interfere with blood flow, they commonly lead to the formation of blood clots. These clots may plug arteries at the site of the plaque or travel elsewhere in the circulation. Sometimes, plaques rupture or become detached from an arterial wall and become lodged in a smaller, downstream artery. Blockage of arteries by plaques or clots may cause a heart attack, stroke, or other potentially life-threatening cardiovascular event. If blood flow to the kidneys is affected, it may lead to chronic kidney disease.
The process in which plaques form is not yet fully understood, but it is thought that it begins when low-density lipoproteins (LDLs) accumulate inside endothelial cells in artery walls, causing inflammation. The inflammation attracts leukocytes that start to form a plaque. Continued inflammation and a cascade of other immune responses cause the plaque to keep growing. Risk factors for the development of atherosclerosis include hypertension, high cholesterol (especially LDL cholesterol), diabetes, and smoking. The chance of developing atherosclerosis also increases with age, male sex, and a family history of cardiovascular disease.
Treatment of atherosclerosis often includes both lifestyle changes and medications to lower cholesterol, control blood pressure, and reduce the risk of blood clot formation. In extreme cases, or when other treatments are inadequate, surgery may be recommended. Surgery may involve the placement of stents in arteries to keep them open and improve blood flow, or the use of grafts to divert blood flow around blocked arteries.
CORONARY ARTERY DISEASE
Coronary artery disease is a group of diseases that result from atherosclerosis of coronary arteries. Treatment of the diseases mainly involves treating the underlying atherosclerosis. Two of the most common coronary artery diseases are angina and myocardial infarction.
ANGINA
Figure 11.31 Angina is pain in the chest due to reduced blood flow in coronary arteries, so the heart muscle does not receive adequate oxygen.
Angina is chest pain or pressure that occurs when heart muscle cells do not receive adequate blood flow and become starved of oxygen (a condition called ischemia). This is illustrated in Figure 11.29. There may also be pain in the back, neck, shoulders, or jaw — and in some cases, the pain may be accompanied by shortness of breath, sweating, or nausea. The main goals of angina treatment are to relieve the symptoms and slow the progression of the underlying atherosclerosis.
Angina may be classified as either stable angina or unstable angina:
Stable angina is angina in which pain is precipitated by exertion (from brisk walking or running, for example) and improves quickly with rest or the administration of nitroglycerin, which dilates coronary arteries and improves blood flow. Stable angina may develop into unstable angina.
Unstable angina is angina in which pain occurs during rest, lasts more than 15 minutes, and is of new onset. This type of angina is more dangerous, and may be a sign of an imminent heart attack. It requires urgent medical attention.
MYOCARDIAL INFARCTION
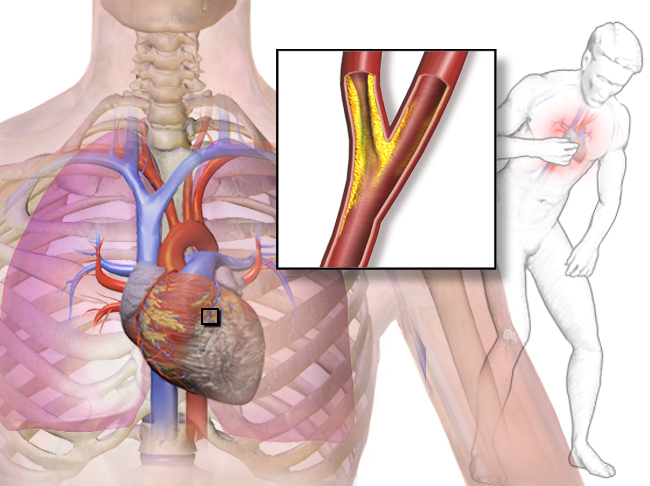
A myocardial infarction (MI), commonly known as a heart attack, occurs when blood flow stops to part of the heart, causing damage to the heart muscle and death of myocardial cells. As shown in Figure 11.32, an MI usually occurs because of complete blockage of a coronary artery, often due to a blood clot or the rupture of a plaque. An MI typically causes chest pain and pressure, among other possible symptoms, but at least one quarter of MIs do not cause any symptoms.
Figure 11.32 A myocardial infarction occurs when cardiac muscle cells die due to blockage of a coronary artery.
In the worst case, an MI may cause sudden death. Even if the patient survives, an MI often causes permanent damage to the heart. This puts the heart at risk of heart arrhythmias, heart failure, and cardiac arrest.
Heart arrhythmias are abnormal heart rhythms, which are potentially life threatening. Heart arrhythmias often can be interrupted with a cardiac defibrillator, which delivers an electrical shock to the heart, in effect “rebooting” it.
Heart failure occurs when the pumping action of the heart is impaired, causing tissues to get inadequate oxygen. This is a chronic condition that tends to get worse over time, although it can be managed with medications.
Cardiac arrest occurs when the heart no longer pumps blood or pumps blood so poorly that vital organs can no longer function. This is a medical emergency that requires immediate intervention.
Hypertension and atherosclerosis often cause other cardiovascular diseases, including stroke and peripheral artery disease.
STROKE
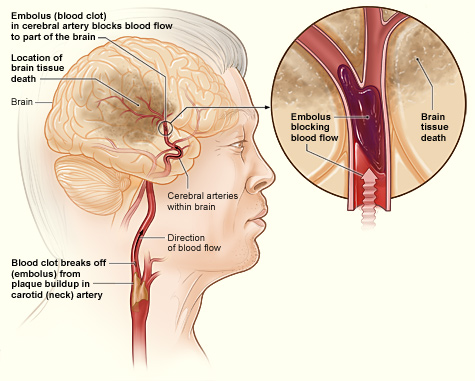
A stroke, also known as a cerebrovascular accident or brain attack, occurs when blocked or broken arteries cause brain cells to die. There are two main types of stroke, both of which are illustrated below: ischemic stroke and hemorrhagic stroke (Figures 11.31 and 11.32).
An ischemic stroke occurs when an blood clot breaks off from a plaque, or forms in the heart because of arrhythmia and travels to the brain, where it becomes lodged in an artery. This blocks blood flow to the part of the brain that is served by arteries downstream from the blockage. Lack of oxygen causes the death of brain cells. Treatment with a clot-busting drug within a few hours of the stroke may prevent permanent damage. Almost 90% of strokes are ischemic strokes.
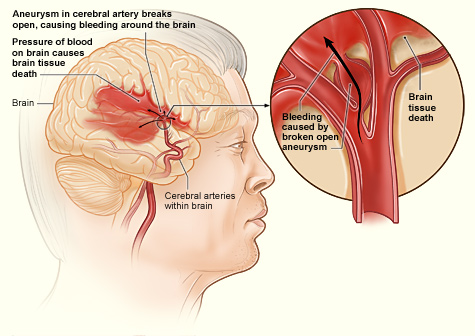
A hemorrhagic stroke occurs when an artery in the brain ruptures and causes bleeding in the brain. This deprives downstream tissues of adequate blood flow, and also puts pressure on brain tissue. Both factors can lead to the death of brain cells. Surgery to temporarily open the cranium may be required to relieve the pressure. Only about ten per cent of strokes are hemorrhagic strokes, but they are more likely to be fatal than ischemic strokes.
Figure 11.33 In an ischemic stroke, brain cells die due to a blocked artery in the brain.Figure 11.34 In a hemorrhagic stroke, brain cells die due to bleeding in the brain. In the example shown here, bleeding occurs when a cerebral artery aneurysm (localized bulge in the wall of a blood vessel) breaks open.
In both types of stroke, the part of the brain that is damaged loses is ability to function normally. Signs and symptoms of stroke may include an inability to move, feel, or see on one side of the body; problems understanding speech or difficulty speaking; memory problems; confusion; and dizziness. Hemorrhagic strokes may also cause a severe headache. The symptoms of stroke usually occur within seconds or minutes of the brain injury. Depending on the severity of the stroke and how quickly treatment is provided, the symptoms may be temporary or permanent. If the symptoms of a stroke go away on their own in less than an hour or two, the stroke is called a transient ischemic attack. Stroke is the leading cause of disability in the United States, but rehabilitation with physical, occupational, speech, or other types of therapy may significantly improve functioning.
The main risk factor for stroke is high blood pressure. Keeping blood pressure within the normal range, whether with lifestyle changes or medications, is the best way to reduce the risk of stroke. Another possible cause of stroke is the use of illicit drugs, such as amphetamines or cocaine. Having had a stroke in the past also greatly increases one’s risk of future strokes. Men are more likely than women to have strokes.
PERIPHERAL ARTERY DISEASE
Figure 11.35Peripheral artery disease typically causes pain and other symptoms, because of decreased blood flow in the leg or other areas of the body served by peripheral arteries.
Peripheral artery disease (PAD) is a narrowing of the arteries other than those that supply the heart or brain, due to atherosclerosis. Figure 11.35 shows how PAD occurs. PAD most commonly affects the legs, but other arteries may also be involved. The classic symptom is leg pain when walking, which usually resolves with rest. This symptom is known as intermittent claudication. Other symptoms may include skin ulcers, bluish skin, cold skin, or poor nail and hair growth in the affected leg(s). Up to half of all cases of PAD, however, do not have any symptoms.
The main risk factor for PAD is smoking. Other risk factors include diabetes, high blood pressure, and high blood cholesterol. The underlying mechanism is usually atherosclerosis. PAD is typically diagnosed when blood pressure readings taken at the ankle are lower than blood pressure readings taken at the upper arm. It is important to diagnose PAD and treat the underlying atherosclerosis, because people with this disorder have a four to five times higher risk of myocardial infarction or stroke. Surgery to expand the affected arteries or to graft vessels in order to bypass blockages may be recommended in some cases.
What is cardiovascular disease? How much mortality do cardiovascular diseases cause?
This condition occurs when blood flow to the heart muscle is stopped causing death of cardiac muscle cells: _______________.
This condition is characterized by consistent elevated blood pressure: ____________________.
This condition consists of chest pain due to heart cells not receiving enough oxygen: ____________________.
This condition is characterized by stiffening of artery walls due to a plaque buildup: ____________________.
List risk factors for cardiovascular disease.
What is coronary artery disease? Identify two specific coronary artery diseases.
Explain how a stroke occurs, and how it affects the patient.
Describe the cause of peripheral artery disease.
What are the similarities between angina and ischemic stroke?
How can kidney disease be caused by problems in the cardiovascular system?
FEATURE: MY HUMAN BODY
You read in this section about the many dangers of hypertension. Do you know if you have hypertension? The only way to know for sure is to have your blood pressure measured. Measuring blood pressure is quick and painless, but several measurements are needed to accurately diagnose hypertension. Some people have what is called “white coat disease.” Their blood pressure rises just because they are being examined by a physician (in a white coat). Blood pressure also fluctuates from time to time due to factors such as hydration, stress, and time of day. Repeatedly measuring and recording your own blood pressure at home can provide your doctor with valuable diagnostic data. Digital blood pressure monitors for home use, like the one in Figure 11.36, are relatively inexpensive, easy to use, and available at most pharmacies.
Figure 11.36 This personal blood pressure monitor is worn on the wrist.
If you do have high blood pressure, lifestyle changes with or without medications can usually bring it under control. A commonly recommended lifestyle change is the adoption of a healthier eating plan, such as the DASH (“Dietary Approaches to Stop Hypertension”) diet. This diet was developed specifically to lower blood pressure without medication. Numerous studies have found the DASH diet to be effective at reducing not only high blood pressure, but also the risk of coronary artery disease, heart failure, stoke, some kinds of cancer, and diabetes. This diet has also been found effective for weight loss. The DASH diet includes whole grains, fruits and vegetables, low-fat or nonfat dairy, lean meats, fish and poultry, beans, nuts, and seeds.
CASE STUDY: FLIGHT RISK
Nineteen-year-old Malcolm is about to take his first plane flight. Shortly after he boards the plane and sits down, a man in his late sixties sits next to him in the aisle seat. About half an hour after the plane takes off, the pilot announces that she is turning the seat belt light off, and that it is safe to move around the cabin.
The man in the aisle seat — who has introduced himself to Malcolm as Willie — immediately unbuckles his seat belt and paces up and down the aisle a few times before returning to his seat. After about 45 minutes, Willie gets up again, walks some more, then sits back down and does some foot and leg exercises. After the third time Willie gets up and paces the aisles, Malcolm asks him whether he is walking so much to accumulate steps on a pedometer or fitness tracking device. Willie laughs and says no. He is actually trying to do something even more important for his health — prevent a blood clot from forming in his legs.
Willie explains that he has a chronic condition: heart failure. Although it sounds scary, his condition is currently well-managed, and he is able to lead a relatively normal lifestyle. However, it does put him at risk of developing other serious health conditions, such as deep vein thrombosis (DVT), which is when a blood clot occurs in the deep veins, usually in the legs. Air travel — and other situations where a person has to sit for a long period of time — increases the risk of DVT. Willie’s doctor said that he is healthy enough to fly, but that he should walk frequently and do leg exercises to help avoid a blood clot.
During the flight, Willie got up to take frequent walks, and was doing leg exercises to try to avoid the medical condition — deep vein thrombosis (DVT). DVT occurs when a blood clot forms in a deep vein, usually in the leg. It can be very dangerous — even deadly.
A blood clot is an aggregation of thrombocytes and proteins. Blood clots are helpful for preventing blood loss when a blood vessel is damaged. In some situations, though, they can be extremely dangerous. Blood clots can cause heart attacks or strokes by blocking the flow of blood to the heart or brain, respectively.
When DVT occurs, one of the major risks is pulmonary embolism (PE). PE is when the blood clot breaks off, travels through the blood vessels, and lodges in a pulmonary artery. Recall what the pulmonary arteries do — they carry deoxygenated blood from the heart to the lungs, where the blood picks up oxygen and releases carbon dioxide due to gas exchange between the capillaries and the alveoli of the lungs. Imagine what would happen if this flow of blood to the lungs was partially or completely blocked by a blood clot. Depending on the size of the blood clot and where it is lodged, a PE can cause a variety of serious consequences, ranging from lung damage to instant death, because of the disruption of the pulmonary circulation.
Willie has a higher risk of DVT and its consequences because he has heart failure. As you have learned, heart failure is a chronic condition in which the pumping action of the heart is impaired. One reason that heart failure is thought to increase the risk of DVT is because the blood is not being pushed strongly enough through the cardiovascular system, allowing blood clots to form more easily.
Willie needs to be particularly concerned about DVT while on a long plane flight. Why do you think this is? Think about how blood flows through arteries and veins. Blood is pushed through arteries mainly due to the pumping action of the heart. Veins, on the other hand, rely on the movement of the surrounding skeletal muscles to help push blood through them. Sitting still for long periods of time in cramped quarters (such as on a plane) can cause blood to pool in the deep veins of the legs, leading to the formation of a blood clot.
Even people who are generally healthy and don’t have heart disease can get DVT from sitting for too long on a long-distance flight, or in other situations when they are immobile for extended periods of time. Fortunately, walking periodically and doing some simple leg exercises can lower your risk of DVT by helping to push blood through your veins. If you are planning on taking a flight in the future, watch the short video below to learn some easy exercises that you can do right in your plane seat to help prevent DVT!
Attributions
This chapter is composed of text taken from of the following sources: